PsoriasisVulgarisMicrograph.jpg
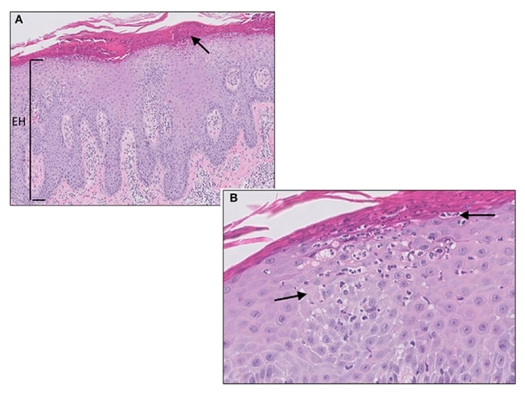
Micrograph of psoriasis vulgaris. Confluent parakeratosis, psoriasiform epidermal hyperplasia [(A), EH], hypogranulosis, and influx of numerous neutrophils in the corneal layer [(A), arrow]. (B) Transepidermal migration of neutrophils from the dermis to the corneal layer (arrows).
I will make no apology for the technical material that is to be read in this chapter. Those with Psoriasis will be happy to use a dictionary to better understand their terrible affliction, and in any case, it is sure that this chapter will be brought to a physician for interpretation and use. That physician will want more than lay language.
The treatment protocol for Psoriasis is simple, and can be read without difficulty.
Brief background
In July of 1986 The Arthritis Trust of America/The Rheumatoid Disease Foundation brought to its Second National Medical Seminar, Dr. Helmut Christ, M.D. of Bisingen, West Germany, as a speaker.
One of Dr. Christ’s subjects was “Psoriasis Under Control at Last.”
Gus J. Prosch, M.D., referral physician, was the first to try this new treatment on a patient with success. He obtained Psoriasis medicines from a pharmacy in Germany recommended by Dr. Helmut Christ.
Dr. Prosch’s patient had tried everything possible, and he had reached a point of suicidal intent if this next treatment did not help, such was his despair.
Prosch proceeded with a successful trial.
On page 138 of "The Art of Getting Well," Helmut Christ, M.D. reported 100% successes.11
Helmut, an Internist-physician who wished to be a general practitioner, and did not choose to be a specialist on Psoriasis, as of this writing has treated 4.000 patients with Psoriasis, mostly by referral from successful patients and physicians. He did not invent the treatment, but rather received it from another physician who had had Psoriasis himself, and eventually developed the successful treatment protocol which has been tested in several universities and clinics.
It should be clear from the start that “Fumaric Acid” per se, is useless, but that “Fumaric Acid Monoethylester” and “Fumaric Acid di-Methylester” are the proper medicines.
There are those who sell “Fumaric Acid” alone for this treatment thereby misleading with a substance that will be of no effect whatsoever.
What is psoriasis?
There are many forms of psoriasis, a skin disease characterized by the formation of scaly red patches on the extensor (following the muscles that perform extension) surfaces of the body.
- Annularis – Psoriasis in ring-shaped patches
- Arthropathica – A form associated with chronic arthritis
- Buccalis – Marked by white, thickened patches in mucuous membrane of cheeks, gums, tongue
- Circinata – See Annularis above
- Diffusa – Coalescence of large contiguous lesions (Bakers, grocers’, bricklayers itch, etc.)
- Discoides – Occurring in solid patches
- Figurata – Lesions in curved linear patterns
- Follicularis – Small, scaly lesions located at openings of sebaceous and sweat glands
- Guttata – Occurs in small, distinct, irregular patches
- Gyrata – Having serpentine arrangement
- Inveterata – with confluent lesions and thickening and hardening skin
- Linguae – See Buccalis above
- Nummularis – In circular patches that resembles coins
- Osteacea – In old, thick, tough patches covered with scales resembling outside of oyster shells
- Palmaris et plantaris – Syphiloderm of palms or soles
- Punctata – Lesions consist of minute, red, pinhead-shaped papules, often surmounted with pearly scales
- Pustular p. – Lesions are covered with pustules
- Rupioides – Rupia-like crusts (skin eruptions usually from syphilis)
- Universalis – Lesions over whole body
As one can easily see, these complex Latin terms are simply means for classifying various views of a skin condition and are not at all meaningful for the purpose of treating and controlling the disease except in certain few cases, such as Rupioides, which seems to be related to a known germ.
If you are one who suffers from Psoriasis, surely you know more about your symptoms than simply how to describe it. You know that it flares up worse then gets better from time to time, that it sometimes can create great embarrassment, pain, guilt – in short, it can indeed control your life.
According to Helmut Christ, M.D.: “It has now been established, that Psoriasis is not a SKIN DISORDER strictly speaking, but a T-cell-mediated autoimmune disease. The problem lies in the subcutaneous immune system. It is not a metabolic disorder as previously thought. It is an inherited disorder and is frequently brought on by factors like streptococcal infections, operations, antibiotics, depression, death of a family member and food-stuffs (spices, nuts, alcohol, chocolate, orange juice).”
We know that patients with Psoriasis have a higher incidence of Rheumatoid Diseases than others.
What is psoriasis?
Simply, it is a hyperproliferation (overgrowth) of the epidermis (outer skin covering), and the cell division is an enhanced 8-10 times normal.
Traditional treatments
Many treatments are directed at interference with DNA synthesis and interruption of cell division as it is presumed this function is in error in our bodies.
Some patients move to warmer climates to increase sun exposure and humidity, although overexposure to sunlight can also aggravate the condition.
The traditional treatments for psoriasis include topical tars and ultraviolet light, keratolytics, anthralin and glucocorticosteroids. Current systemic therapies using psoralen-photochemotherapy or methotrexate are still largely investigational and may produce adverse effects. Besides blocking the abnormal rapid proliferation of psoriasis, methotrexate affects other normally rapidly growing tissues such as bone marrow, gastrointestinal tissues and hair roots.
Fluorinated steroids may be useful on a short-term basis for treatment of resistant, highly inflamed, or irritated plaques, but are not advisable for treatment of widespread psoriasis. Hydrocortisone creams are commonly used with mixed results for intetriginous (chafed) areas or on the face since they do not atrophy the skin. However, systemic steroids are generally contraindicated, as cessation is usually accompanied by rebound worsening of the disease.
PUVA (Psoralen and long-wave ultraviolet light) have been useful therapies but are still investigational. Side effects include phototoxicity with erythema and blistering, pruritis and nausea. Potential chronic side effects such as actinic damage and aging of the skin, carcinogenesis and cataract formation are of great concern. Moreover, patient compliance is generally poor. An average of 25 treatments given 2 or 3 times weekly are required for 80% clearing of Psoriasis. Patients who work outdoors do not like to wear goggles. Psoralen and long-wave ultraviolet light (PUVA) is only a palliative treatment and requires continued maintenance therapy. At Stanford University, experience with PUVA has shown that over 90% of patients develop recurrent psoriasis in the first year of therapy.
Crude coal tars, often combined with zinc and salicylic acid, has been a valuable adjunctive treatment for psoriasis. Coal tar products are able to suppress DNA synthesis in the epidermis within the first few hours after application. The Goeckerman regimen, combining coal tar with exposure to UV light, has induced remissions for several weeks and is a relatively safe method. Patient compliance is still a problem as these tars are messy and stain clothing. Some patients develop acanthomas (tumor or excessive development of skin). Coal tars also produce folliculitis (inflammation of hair folliculs). The absorbed mutagens may increase the risk of some forms of cancer. Crude coal tar is a mixture of 10,000 non-standarized components, which may create a potential problem of contact allergic sensitization.
The synthetic retinoids are a major advance in the treatment of both localized as well as generalized pusular Psoriasis. The dosage must be carefully monitored, as some patients experience a local recurrence of pustules with the lowered dosage. All of the important factors concerning toxicity and side effects of these drugs need to be considered carefully, especially the teratogenic effects. Some of the side effects are dose-dependent (e.g. dryness of the lips and oral mucosa) and are reversible after discontinuation of therapy. Other side effects include exfoliation (a falling off in scales or layers) of palms and soles, hair loss, conjunctivitis (inflammation of the layer that lines the eyelids), pruritis, paronchia, elevated serum lipids, muscle pain, neuralgia and hyperostosis (bone disorder). Considering the possible long-term effects of retinoid-induced lipid modulation on atherosclerosis and coronary artery disease, it is necessary to closely monitor the levels of serum lipids during therapy, particularly in patients with CHD risk factors. Some of the non-toxic therapies which may be used prophylactically in patients treated with retinoids include niacin (400 mg b.i.d) and L-Carnitine (250 mg b.i.d.).
Methotrexate is often used as a third-line therapy for patients with severe psoriasis (e.g. acute pustular Psoriasis, Psoriatic Arthritis, Psoriatic Erythroderma) unresponsive to other, less toxic therapies. Liver and renal functions must be carefully monitored prior to treatment. Severe liver disease, such as fibrosis and cirrhosis, may be present in patients with Psoriasis, especially in alcoholics. Unfortunately, no liver function tests are reliable indicators of severe liver toxicity. Other risk factors include obesity, diabetes and lowered renal function. One can minimize the risk by titrating the patient to the lowest possible dose to achieve and maintain adequate control, rather than 100% clearing of the Psoriasis. Like many other treatments for Psoriasis, methotrexate is a known teratogen.
Recently ointments containing pimecrolimus and tacrolimus have been used which have an immunmodulating affect on the T-cells in the dermis.
Regardless of the treatment used, patient education remains a critical component in the successful management of Psoriasis. Therefore patient education manuals and even support groups will enhance the prognosis of the disease and may even strengthen the base of patient referrals to a dermatologist’s practice. Patients should be advised on those factors which make Psoriasis worse. Trauma and irritation of the skin, induced by rubbing, scratching or scrubbing off scales all can produce Psoriasis. Some throat and upper respiratory infections may flare Psoriasis and should be promptly treated by a physician. Some dermatologists are so absorbed in their subspecialty that they overlook the common patient complaints, normally encountered by a general practitioner (e.g. strep infections). Guttate Psoriasis (lesions that are drop shaped) particularly occurs in children and adolescents after strep infections.
Patients should be encouraged to discuss other illnesses besides their chief complaint. Most patients do not understand the fact that sun exposure should be used in moderation. While sunlight in moderation usually helps Psoriasis, sunburn may cause Psoriasis to flare up. A similar situation exists with topical steroids. Patients should be advised not to use these creams on areas in which the Psoriasis is cleared and to follow their dermatologist’s directions carefully to preclude a rebound phenomenon. Stress and anxiety should be minimized. Dietary recommendations are outlined in conjunction with our recommended treatment which is also the new European fumaric acid protocol.
Recent evidence points to abonormalities in the arachidonic acid metabolism in patients with Psoriasis. The cyclic AMP/cyclic GMP ratio is decreased in involved epidermis of Psoriasis compared with uninvolved epidermis from Psoriasis patients or epidermis from normal volunteers. The imbalance of the two cyclic nucleotides plays a central role in the pathogenesis of Psoriasis. Usually, tissue levels of free fatty acids are quite low. However, involved epidermis of Psoriasis contains high concentrations of free arachidonic acid. Elevated levels of the prostaglandin series leads to increased platelet aggregation. Fish oils, high in eicosapentaenoic acid and docosahexaenoic acids (EPA & DHA) are currently being used for normalizing aberations in the arachidonic acid cascade. It is interesting to note that the majority of patients with Psoriasis have elevated levels of cholesterol and triglycerides which may result from abnormal platelet behavior. Epidermal cells in Psoriatic lesions have a receptor for serum beta-lipoproteins. The rate of epidermal lipid synthesis may be regulated by serum lipoproteins. Dermatologists are encouraged to observe and control lipid abnormalities with Psoriasis.
One very promising treatment for Psoriasis is based on the use of fumaric acid ester. Clinical investigations with fumaric acid, an unsaturated dibasic acid, have been conducted in University Medical Centers in Switzerland, West Germany, Japan and the Netherlands and the results are promising. Fumaric acid is the transisomer of malic acid and an intermediate in the Krebs citric acid cycle. Fumaric acid ester has been used both topically and orally and a titration protocol has been suggested.
Rationale for use of fumaric acid ester
Psoriasis is regarded as a disease having its origin in the immunsystem. A defect of fumaric acid metabolism is unlikely. Fumaric acid is the transisomer of malic acid. It is an important compound biochemically since it enters into the citric acid cycle. Fumarate is a by-product at certain stages in the arginine-urea cycle and in purine biosynthesis. Since the citric acid cycle is the center for energy production with the cell, fumaric acid must be present in every cell of the body as it is a by-product of the cycle. Although fumaric acid is not a foreign substance, it is metabolically very active.
In healthy individuals, fumaric acid is formed in the skin when it is exposed to sunlight (from the ultra-violet part of the spectrum). Apparently, patients suffering from Psoriasis have a biochemical defect in which they cannot produce enough fumaric acid and need prolonged exposure to the sun to produce it. This is one reason why patients frequently notice an improvement of their skin condition in the summer months and also explains, in part, the efficacy of PUVA treatment.
This protocol for the treatment of Psoriasis with fumaric acid capsules is based on several clinical studies conducted at the Beau Reveil Clinic in Leysin, Switzerland and the West End Hospital in den Haage, Netherlands. Studies were reported in the following journals: Ned. Tijdschr. Geneeskd., Gann, Med. Msch., Biochem. Pharm., Arch. Derm. Res. and Arch. Derm. Forsch.
Further references follow at the end of this article, but hereafter I shall follow the protocol as presented by Helmut Christ, M.D. and used by Gus Prosch, Jr., M.D. and other referral physicians of The Rheumatoid Disease Foundation.
Psoriasis Treatment Protocol from Helmut Christ, M.D.
In healthy individuals, fumaric acid is formed in the skin when it is exposed to sunlight (from ultra-violet part of the spectrum). Apparently the patient suffering from Psoriasis cannot make fumaric acid that easily, so that he suffers a lack of the acid and needs a longer exposure to the sun to produce it. This is why these patients frequently notice an improvement of their skin condition in the summer months. The aim of our treatment is therefore not only the application of ointments and creams on the skin or its exposure to ultra-violet light, but the careful oral administration of the lacking fumaric acid. This is the basis of our treatment. At no time is the patient treated with cortisone, either by mouth or on his skin. (The patients frequently come from Dermatologists or University clinics, having been treated for years with Cortisone orally or as part of the ointment.)
What is fumaric acid?
Chemically it is an unsaturated dicarbonic acid and is part of the citric acid cycle.
CH - COOH
| |
CH - COOH
As the citric acid cycle is the center for energy production within the cell, fumaric acid must be present in every cell of the body, being a by-product of the cycle. It is therefore not something that is foreign to the body. A lack of fumaric acid leads to the accumulation of half-products. These products, we believe, are responsible for the skin lesions in patients with Psoriasis. In administering the lacking fumaric acid slowly to the body, the Psoriasis can come to a halt. The administration of the acid should be slow, as it is a metabolically very active substance. However the administration of too little fumaric acid ester will result in a therapeutic failure, whereas too much can lead to heat waves and a drop in blood sugar. This is a very rare occurrence.
The patient with Psoriasis may eat and drink everything that does not produce itching of the skin.
The rule is: If it itches today, then there was something in the food yesterday that his/her skin cannot tolerate. In this way every patient must eventually find out for themself what foods and spices their skin can tolerate and what foods should be avoided. I find it amazing that no Dermatologist or Skin clinic advises the patients in this way, but if one takes a careful history, the doctor will discover that many patients avoid certain food stuffs. A guideline for allowed foods is included.
Other factors which can trigger off a relapse in the skin condition are acute illnesses accompanied by high temperatures, and conditions accompanied by accumulation of pus, like purulent tonsillitis, skin abscesses, root-abcesses of teeth, mycotic infections, cellulites, pyorderma, etc. These should be treated immediately and vigorously.
It is adviseable that the patient exercise frequently (jogging) and really sweat.
Treatment Protocol
Fumaric Acid Ester Tablets (Strength I and II):
At the end of every evening the patient should take his tablet with a lot of fluid either tea, mineral water or preferably milk as this will reduce stomach acidity. If the patient gets an uneasy epigastric feeling after about an hour, he should take the capsule with a little sugar, as the blood sugar may drop a little at this time. (Of course diabetic patients will experience an improvement of their diabetic state – watch the fasting blood sugar a little more carefully.) The patient should not take the fumaric acid ester with coffee as this will increase gastric acidity, and cause more epigastric discomfort. If he wants to he can also take the tablet dissolved. After about 15 to 30 minutes he will notice a warm feeling and a tingling of the skin, the shoulder, and neck region up to the ear lobes. This reaction lasts approximately half an hour. This indicates that the metabolic process has started. Very rarely the reaction can also come on several hours after taking the tablet and occasionally it may be felt over the whole body. School children should be watched a little more carefully and should carry sweets with them, as they may experience a slight fainting after about 2 to 3 hours from a drop in blood sugar.
The fumaric acid ester tablets are the basis of the treatment, and they actually affect pH in the digestive tract, resulting in better digestion of foods. It is important for every patient to find out the right dose of fumaric acid ester that he needs to keep his skin clear. The dosage may be very variable. If a certain dose does not lead to an improvement of the skin, he should increase the number of tablets every 2 to 3 weeks by ONE tablet (capsule) only. As long as he experiences a warm or tingling feeling in the neck and shoulders or as long as the lesions are slowly subsiding, he can stick to the same dose.
Fumaric Acid Ester Ointment
A compounding pharmacist will prepare this ointment for you. It should be used if the lesions are localized or confined only to the elbows and knees. Very small amounts should be rubbed into the skin lesions daily. An erythema (morbid skin redness) after the application is a good sign. DO NOT apply bandages together with the ointment – else the erythema will be very severe and the skin will burn. One may alternate the fumaric ointment with a salicylic acid ointment if the skin reaction is severe. Rub the ointment only on small areas and only on lesions which appear most active. If the skin tends to become very dry, apply a fattening ointment.
Fumaric Acid Ester Bath
Please notice that this solution should not be added to the bath, but also applied to the skin. The bottle should be mixed well before use. If the patient has very diffuse lesions over the whole body, he should use this solution and rub it very sparingly into the skin and wait for approximately 10 minutes (while the bath is being filled). The water should not be too hot and the bath should not last longer than about 15 minutes. When the lesions begin to subside, the ointment should be used for the remaining areas as described above.
Fumaric Acid Lotion
In West Germany Dr. Christ is using a lotion that is rubbed into the scalp immediately after washing the hair, so that it becomes diluted a little – else a slight burning sensation may occur. According to Christ, it is (translated from the German the best possible at this writing):
Fumaric Scalp Lotion Prescription (FS-Lotio)
- (RP!) Fumaric Acid 4.0
- Monoethyl fumarate 4.0
- Infiltrina 10.0 (Something to cause infiltration of scalp, like DMSO – dimethylsulfoxide, perhaps)
- Solutio Cordes ad 100.0
- MDS. (Place Where It is To Be Used): Scalp
- Lotion (Kopfhaut-Lotio)
General Measures
The natural course of the illness is one of remissions and relapses. If possible the patient should avoid stressful situations.
Dr. Christ suggests that any patient who is seriously interested in getting rid of Psoriasis, to drink absolutely no alcohol, at least until the skin is clear. If the patient’s skin does not recover within a few weeks, he suggests to give the patient liver tablets, especially those metabolic products which are found in the fumaric acid cycle (L-Arginine, L-Citrulline, L-Aspartate and L-Ornithine). He would give these in the form of an injection intravenously every day for 2 to 3 weeks. Very frequently the patient will then experience a dramatic improvement of the skin.
It is most important to avoid wines of all kind, as these can produce a relapse. They should also not be used in cooking, gravies, etc.
Nuts of all kinds should be avoided, except almonds. Dissolved aromatic substances in the nuts are the cause of an exacerbation. Peanuts and products made of them (e.g. butter) must be strictly avoided, also mustard, pepper, curry, etc.
Most important for the treating physician to remember:
- Always start the treatment with fumaric acid ester tablets of low concentration. Increase the number of tablets slowly, every 2 to 3 weeks. The maximum dose is 2 to 3 tablets of strength III. As long as the patient experiences the warm tingling feeling over the neck and shoulders, or as long as he notices that the skin lesions are slowly subsiding, he need not increase the dose.
- Always remind the patient, that around the 10th to 14th day s/he might experience a slight worsening of itching, or may develop slight edema. This is only transient, if it does occur, and lasts only a few days. If really necessary, you might give a diuretic or antihistaminic preparation; usually it is not a problem.
- The patient should never get penicillin vk. If an infection does have to be treated with an antibiotic, give any other drug except Pencillin VK and watch the patient a little more carefully regarding a relapse. Several other medications will also prevent skin improvement, namely the following ACE-inhibitors: (Angiotensin Converting Enzyme), Calcium-antagonists and beta-blockers, like propranolol.
- Ointments should be applied very thin and should never be covered up (no bandages, no band-aids, etc.).
- It is most important that the patient stick to the diet, at least for 2 to 3 months. Only when the skin has recovered completely, should s/he start adding spices to foods and try different foods to find out what his/her skin will tolerate.
- I would not advise the patient to use ultra-violet light additionally. I doubt whether improvement of the skin is accelerated in this way – and besides, there are several reports from the United States of an increased rate of skin cancer.
- When the skin is clear (no scars are left behind on healing) the patient may slowly try to reduce the number of fumaric acid tablets. If the skin does start to itch again, he must continue with the dose that kept the lesions away.
- Reassure the patient that s/he is taking a harmless medication which is not foreign to his body and has no serious side-effects on the liver, kidney, etc. I reassure the patient by showing him the laboratory data regarding hepatic and renal function.
- If the skin does not clear up, the patient is either not taking his medication correctly (that is too little medication), or s/he is not sticking to the diet, or the diagnosis is incorrect. Mycotic infections may mimic Psoriasis and antimycotic treatment should be tried if the fumaric acid ester treatment does not bring the expected improvement. (Helmut Christ,M.D. says: “I am still waiting for the first patient who does not show an improvement – sometimes it just takes a couple of weeks longer!”)
- Additional recommendations (besides the diet) are that patients should also take Omega-3-fatt acids and Omega-6-fatty acids. This was a chance finding and was published in The Lancet Nr. 8582, p. 378-380.
Dietary Recommendations for Psoriasis
Foods to be avoided
- Meat: Pork
- Spices: All types of aromatic seasoning, pepper, ginger, clove, nutmeg, caraway, anise (licorice), cinnamon, mustard, red pepper, seasoned foods, e.g. sausages, mixed seasoning, (seasoning salt), pre-spiced dishes (e.g. salami, luncheon meats, bouillon cubes), mayonnaise, orange syrup, candied lemon peel, lemon flavoring or extract.
- Nuts: Filberts, Hazelnuts, peanuts, all products made of peanuts, e.g. butter, cakes, etc., peanut oil, walnuts, chocolate with nuts.
- Alcohols: Wines of all sorts, wine-vinegar, cognac, champagne, sherry, vermouth, port, malaga, liqueur, all other alcohols or foods containing alcohols.
Foods Allowed
- Meat: Fish, beef, venison, poultry.
- Fruit: All types, tomatoes, fruit-vinegar.
- Vegetables: All types, rice, potatoes, pasta, cabbages, saffron, legumes (without forbidden spices).
- Spices: garlic, onion, herbs, parsley, chives, peppercorn, etc.
- Oils: olives, olive oil, saffron.
- Nuts: coconuts, almonds, all products made of almonds.
- Pastries: Various kinds.
Highly Recommended
- Hand-pressed fresh fruit juices, lots of beetroot-juice, carrot juice
- Milk products (yogurt, curd)
- Sauerkraut
- Pickles without pepper, half-sour pickles
This diet recommendation is that of both Helmut Christ, M.D. and Clinique Beau Reveil, CH 1854, Leysin Switzerland.
Remember Dr. Christ’s statement: "If the skin does not clear up, the patient is either not taking his/her medication correctly (that is, too little medication), or he/she is not sticking to the diet, or the diagnosis [of Psoriasis] is incorrect."
Psoriasis-Therapy of Dr. med. Schafer and Dr. med. Christ
(Translated the best possible at this writing)
Salve
- Fumaric Acid Monoethylester 1.5
- Skin Cream (DDD*) 15.0
- DMSO (Dimethylsulfoxide) 8.0
- Milk Acid Ethylester ` 1.0
- Glyoxylic Diureide 1.0
- Eucerin anhydric to 50.0
* Skin Cream (DDD) Composition: Salicylic Acid, Camphor, Chlorobutanol, Phenol, Methylsalicylate, Thymol. This is a mixture of substances, in different strengths, available through pharmacies in Germany and England, and with these properties (according to German package insert): “DDD penetrates deep into the skin tissue and, because of its antiseptic and antibacterial force, it fights effectfully inflamation and pus instigators. DDD activates the metabolism process in the skin, promotes the blood circulation and provides better nutrition of the cells, better extraction of disease agitators and promotes the new formation of healthy, hardy tissue. Itching, tension in the skin, and pain sensations disappear most immediately after the application.” (Produced in license of DDD Ltd., England by DDD Lab, 1000 Berlin, 30 Delta Clinic, 6078 New Isenburg.)
Psoriasis-Bath
- Fumaric acid 100 g
- Balneum Herb Bath 500 ml
Taken From the German From Helmut Christ
Fumaric Powder Capsule I
Fumaric Acid Monoethylester – Metal Salts:
- F. - Fe Salt 0.100g
- F. - Ca Salt 0.400g
- F. - Mg Salt 0.400g
- F. - Li Salt 0.200g
- F. - K Salt 0.200g
- F. - Zn Salt 0.400g
- F. - Cu Salt 0.020g
- Fumaric Acid 0.600g
- Fumaric Acid dimethyl Ester 0.600g
These constituents (to go into) 20 capsules. Generally, should be taken after meals, the amount determined by the doctor.
NOTE: For the prescription it is sufficient to use the name “Fumaric Powder Capsule I.” For chronic therapy an amount of 120 capsules is recommended for the prescription.
Fumaric Powder Capsule II
Fumaric Acid Monoetheylester – Metal Salts:
- F. - Ca Salt 1.0g
- F. - Fe Salt 0.12g
- F. - Cu Salt 0.02g
- F. - Mg Salt 0.8g
- Fumaric Acid dimethyl Ester 2.4g
- Magnesium Carbonate 0.8g
- Zincum Oxide 0.2g
These constituents (to go into) 20 capsules. Generally, should be taken after meals, the amount determined by the doctor.
NOTE: For the prescription it is sufficient to use the name “Fumaric Powder Capsule II.” For chronic therapy an amount of 120 capsules is recommended for the prescription.
Fumaric Acid Bath
- Fumaric Acid 100.0
- Balneum Herbal Oilbath 500.0
Usage: As soon as you have wet your body in the shower, you use this bath liquid, and after that use the powder on the skin lesions. After waiting 5 minutes for it to take effect, rinse off the whole body with water.
Fumaric Salve I
- Fumaric Acid Monoethylester 3.0
- Glyoxylic Diureide 3.0
- Lactic Acid Ethyl Ester 3.0
- DMSO 10.0
- DDD – Soothing Skin Cream 40.0
- Eucerin anlydricum to 100.0
Usage: According to instructions of doctor. Fumaric Salve I is for the patient with strong itching.
NOTE: For the prescription it is sufficient to use the name “Fumaric Salve I.”
Helmut Christ, M.D. states that he has had no experience with items 5, 6, and 7 that follow, but they were so interesting, and they might be useful and so I include them.
Fumaric Salve II
- Fumaric Acid Monoethylester 3.0
- Glyoxylic Diureide 3.0
- Decoderm Basis Cream 40.0
- Eucerin With Water to 100.0
Usage: According to instructions of doctor. Fumaric Salve II is only for skin care.
NOTE: For the prescription it is sufficient to use the name “Fumaric Salve II.”
(Scalp) Head Alcohol
- Fumaric Acid 2.5
- Fumaric Acid Monoethylester 2.5
- DMSO 5.0
- Spiritus Cordes to 100.0
Usage: According to instructions of doctor.
Fumaric Fingernail Polish
- Griseofulvin 0.01
- Fumaric Acid Monoethylester 0.5
- Benzoic Acid Ethyl Ester 0.3
- Mallebrin 0.1
- Talcum 0.05
- Cellulose Nitrate Lacquer to 10.0
Usage: According to instructions of doctor.
Over the past 6 years we were able to increase the success rate of the healing effect of the fumaric acid ester by the addition of thymus extract, the trace mineral selenium, zinc and vitamin B complexe as intravenous infusion (see enclosed publication).
The following is an interesting letter from Helmut Christ, M.D. to Robert F. Cathcart, M.D., a copy forwarded to me at Christ’s request, March 1, 1989:
“Thank you very much for your letter dated Dec. 1, 1988. Please excuse the long delay for answering, but as you guessed, I am being flooded with letters from physicians and patients in the U.S. wanting to know more about the treatment [Psoriasis, Ed:] and where they can get the medication.
“It appears that physicians in this country are slowly wakening up and becoming more and more alert to this very successful type of treatment and I just cannot cope any more. I am seriously considering having another physician to assist me.
“Other medications that interfere with the fumaric acid [ester] treatment – this is an interesting subject. I don’t know why Betablockers, Calcium-antagonists and Angiotensin-convertingenzyme inhibitors prevent the psoriatic lesions from healing off. It could be a local effect at the site of the scales on the skin. However I believe that these drugs interfere in metabolic pathways, either in the citric acid cycle or the fumaric acid cycle, which is closely connected to the former. You are reading my thoughts by suggesting that fumaric acid [ester] may act as a type of antibiotic in the bowel killing... organism[s]. How else can you explain that Metronidazole gives some improvement in patients with psoriasis. Maybe one should try both substances in patients – 10% – who just don’t want to get better. One should investigate this problem with bacteriological sensitivity tests.
“Another interesting aspect is that if you give these patients the metabolic products of the fumaric acid cycle, e.g, L-Citrulline, L-Argnine, L-Ornithine, L-Aspartate (The L-amino acids), intravenously you can watch the patient getting better week to week.
“As far as literature [scientific studies] goes, I have a large collection, but it is all in German! I would suggest that you order the capsules, ointment, bath and lotion for the scalp on a regular basis – BUT IN SMALL AMOUNTS – from our pharmacist[s] in Germany. I have heard from several patients in the U.S. that they are getting the fumaric acid [ester] from . . . and some trace minerals and the whole thing doesn’t help the patient at all. The secret is that it is important that the ‘Ester’ form of the fumaric acid has to be used and not fumaric acid as such, alone.”
[I would like to apologize in advance for possible incomplete or mistaken translations of the materials forwarded to us by Helmut Christ, M.D. Perry A. (Tony) Chapdelaine, M.D. is responsible for translations that are presented for which thanks are due. ~Anthony di Fabio, editor.]
References
- Chopra, D.P. & Flaxman, B.A. Comparative proliferative kinetics of cells from normal human epidermis and benign epidermal hyperplasia (psoriasis) in vitro. Cell and Tissue Kinetics. 7.69, 1974.
- Weinstein, G.D. & Frost, P. Abnormal cell profliferation in psoriasis. J. Invest. Derm. 50:254, 1968.
- Schweckendiek, W. Helilung von Psoriasis vlugaris. Med. Msch. 13:103-104, 1959.
- Kuroda, Z. and Akao, M. Antitumor and anti-intoxication activities of fumaric acid in cultured cells. Gann, 72:777-782, 1981.
- Hagedorn, K. et al. Fumarsauremonoathylester: Wirkung auf DNA-Synthese und erste tierexperimentelle Befunde. Arch. Derm. Res. 254:67-73, 1975.
- Bruynzeel, D. Kan fumaarzuur worden toegepast bij psoriasis? Ned. Tijdschr. Geneeskd. 128(35):1677, 1984.
- Petres, J. et al. Der Einfluss von Fumarasuremono-athylester auf die Nucleinsaure-und Proteinsynthese PHA-stimulierter menschlicher Lymphocyten. Arch. Derm. Forsch. 251:295-300, 1975.
- Baron, D. fumaarzuur worden toegpast bij psoriasis (Vraag en Antwoord). Ned. tijdschr. Geneeskd. 128(24):1152-1153, 1984.
- van Dijk, E. Fumaarzuur voor de behandeling van patienten met psoriasis. Ned. Tijdschr. Geneeskd. 129(11):485-486, 1985.
- Kuroda, K. and Akao, K. Reduction by fumaric acid of side effects of Mitomycin C. Biochem. Pharm. 29:2839-2844, 1980.
- Anthony di Fabio, The Art of Getting Well, 1988
I also refer the reader to Townsend Letters for Doctors article “Immunosuppression of Polyunsaturated Fatty Acids in Autoimmune Diseases, Cancer and Heart Attacks” written by Wayne Martin, published July 1988, p. 271.
Sources are given in references. Authors of contributions/quotations are alphabetically arranged; major author, if any, is in bold.
- Robert F. Cathcart, M.D.
- Perry A. Chapdelaine, Jr., M.D. (translations from German)
- Helmut Christ, M.D.
- Goeckerman
- Wayne Martin, B.S.
- Gus J. Prosch, Jr., M.D.
- Anthony di Fabio, responsible editor/writer
Copyright 1990. All rights reserved by The Roger Wyburn-Mason and Jack M. Blount Foundation for the Eradication of Rheumatoid Disease AKA The Arthritis Trust of America.® The Rheumatoid Disease Foundation / The Arthritis Trust of America was dissolved in 2020 and all website content was transferred to the Foundation for Alternative and Integrative Medicine.

{kind=link}