Chapter 20 of "Energetics and Spirituality" by Lyn Freeman
beverlyrubik.jpg

Beverly Rubik, Ph.D.
Energy medicine is one of the major categories of complementary and alternative medicine (CAM). These therapies typically involve low-level energy field interactions. They include human energy therapies, homeopathy, acupuncture, magnet therapy, bioelectromagnetic therapy, electrodermal therapy, and phototherapy, among others.
Many of these modalities challenge the dominant biomedical paradigm because they cannot be explained by the usual biochemical mechanisms. One possible influence of biofield phenomena is that they may act directly on molecular structures, changing the conformation of molecules in functionally significant ways. Another influence is that they may transfer bioinformation carried by very small energy signals interacting directly with the energy fields of life, which is more recently known as the biofield (Rubik et al, 1994).
Moreover, other mysteries in biology and medicine exist that appear to involve interacting energetic fields, including the mystery of regenerative healing in animals, sometimes associated with innate electromagnetic energy fields that have been measured (Becker, 1960, 1961) and sometimes actually stimulated with external low-level energy fields (Becker, 1972; Smith, 1967). Another mystery is that living organisms respond to extremely low-level nonionizing electromagnetic fields, displaying a variety of effects ranging from cellular and subcellular scales to the level of brain, emotions, and behavior. These fields may be beneficial (therapeutic), deleterious (electromagnetic pollution), or neutral. Then, the mystery of embryonic development from the fertilized egg to an organized integral animal should be considered, which may also involve innate energy fields, starting with the initial polarization of the fertilized egg.
Although these phenomena involve an integral and dynamic wholeness that challenge the power of molecular explanation, another biophysical view of life has been offered that may help explain them. Living systems may be regarded as complex, nonlinear, dynamic, self-organizing systems of energetic and field phenomena. At the highest level of organization, each life form may possess an innate biologic field, or biofield, a complex, dynamic, weak energy field involved in maintaining the integrity of the whole organism, regulating its physiologic and biochemical responses, and integral to development, healing, and regeneration (Rubik, 1993, 1997, 2002b).
Needless to say, the concept of an organizing field in biology and medicine evokes shades of vitalism, an old philosophical concept in the West from the 1600s that was overthrown in nineteenth-century science. In this view, the essence of life is seen as a metaphysical, irreducible life force that cannot be measured. Indigenous systems of healing such as Ayurvedic and Chinese medicine and modern modalities such as chiropractic rest on concepts of a vital force or subtle life energy that is central to healing. Called by many names, including prana in Ayurvedic medicine and qi in Chinese medicine, these indigenous terms go back thousands of years. They may actually refer to something similar to the present-day concept of the biofield, which is, at least in part, based on the electromagnetic field theory of modern physics but, in principle, might also include acoustic and possibly other subtler energy fields not yet known to science. The important difference between traditional and modern views of the vital force is that the biofield rests on physical principles and can be measured, whereas the traditional concepts remain metaphysical. Nonetheless, considerable similarities exist between ancient concepts of the life force and modern biofield concepts in their assumption that a form of life-giving energy flows throughout the body and that illness arises as a result of blockages, excesses, or irregularities in its flow. Additionally, biofield therapies incorporate notions of a universal life energy, as in Reiki (a form of Japanese spiritual healing), qigong therapy, and many other types of human energy healing performed today. Many practitioners of biofield therapies can also assess imbalances in the human biofield either with their hands or intuitively.
On the one hand, an organism is similar to a crystalline structure of ordered biomolecules. On the other hand, the essence of life is more similar to a flame, burning matter into energy and dancing not only with organized vitality, but also with an element of unpredictability or chaos. Both views may be necessary to describe life in the same way that, in quantum physics, both a particle view and a wave view are necessary to describe fully the nature of light, as well as matter at the smallest scales. This dual model in physics, popularized by the Copenhagen interpretation of quantum theory, is called the principle of complementarity. Similarly, an energy field view of life may be seen as complementary to the conventional biomolecular view rather than antagonistic. The brain, for example, can be analyzed in terms of the receptors, neurotransmitters, ion channels, and so forth that help explain neuronal firing; or it can be viewed in terms of the oscillations of its neuronal circuits and the magnetic and electrical fields of its continual activity, with possible regulatory feedback from the fields themselves. The biophysical foundation of life, proposed here as the biofield, provides the rudiments of a scientific foundation for understanding some of mysteries of life that remain and may perhaps take us beyond into a new era of understanding life.
Electromagnetic Fields in Life
Electrical currents, along with their associated magnetic fields, can be found in the body (Becker and Selden, 1985). The electrical and magnetic fields of the human body are complex and dynamic and are associated with dynamical processes such as heart and brain function, blood and lymph flow, ion transport across cell membranes, and many other biologic processes on many different scales. These phenomena all contribute various field components to the biofield.
In addition, a broad spectrum of radiant energies exists known as electromagnetic waves, ranging from the ultra-low, extremely low, very-low, low, and medium broadcast waves; very high – frequency broadcast waves; microwaves; infrared rays; visible light rays; and even ultraviolet radiation, all emanating from the human body. The peak intensity of the electromagnetic radiation of the human biofield is in the infrared region of the electromagnetic spectrum, in the range of 4 to 20 microns in wavelength. The belief is that much of this emission, particularly in the infrared region, is from thermal effects associated with metabolism.
Human Biofield
The human body emits low-level light, heat, and acoustical energy; has electrical and magnetic properties; and may also transduce energy that cannot be easily defined by physics and chemistry. All of these emissions are part of the human energy field, also called the biologic field, or biofield. However, no agreement has been reached in the scientific community on the definition of the biofield. Various approaches have been submitted by this author (Rubik, 1993, 1997, 2002b) and other authors [Popp (1996); Tiller (1993); Welch (1992); Welch and Smith (1990); and Zhang (1995, 1996)]. Most research has focused on electromagnetic aspects of the biofield. We restrict the rest of this chapter to the electromagnetic portion of the human biofield where the main scientific focus has been.
Biology has been preoccupied with its molecular revolution that focuses on structure-function relationships in biochemistry. This effort culminated in the Human Genome Project whereby teams of scientists from around the world mapped all the genes in human deoxyribonucleic acid. Most of the scientific effort and funding remains in molecular biology. By contrast, only a small number of scientists worldwide have worked to understand the energy fields of the human body. Moreover, measuring the biofield and understanding its role in life are more difficult than the study of more tangible phenomena, and the funding for the former has been extremely scarce. Therefore scientific advances in biofield research have been few, and biofield science remains a frontier area ripe for exploration.
"If we try to pick out any thing by itself, we find it hitched to every thing else in the universe"
~ John Muir, 1911
The biofield is also elusive. We cannot isolate it or analyze it comprehensively. As John Muir wrote, "if we try to pick out any thing by itself, we find it hitched to every thing else in the universe" (Muir, 1911). For a field, this connection is especially true, given that, regardless of its source, it travels outwards to infinity, interacts with other fields by superposition, and interacts with matter along the way. Additionally, phenomena such as resonance can occur, involving an energetic coupling of, or oscillation within, matter. The fields of the human body may also be influenced by the fields of nearby organisms, the biosphere, and even the earth and cosmos, especially geocosmic rhythms. From a theoretical perspective, we cannot calculate the human biofield from first principles because of its dynamic aspects and enormous complexity. Nonetheless, we can measure certain aspects of the biofield and observe its footprints via novel technologies.
The human biofield may carry novel information of diagnostic and predictive value for medicine. Thus new technologic developments and methodologic improvements in measuring the biofield should be a central aim of health-related research. By measuring various aspects of the biofield, we may be able to recognize organ and tissue dysfunctions even in advance of diseases or symptoms and treat them appropriately so as to eradicate them. We may also be able to use biofield measurements to predict whether the effect of a particular course of therapy will be effective or ineffective, depending on whether it improves or thwarts the biofield. This possibility is especially true for the CAM therapies, which, in principal, often evoke a shift in response to extremely small stimuli that harmoniously work with the human body’s natural dynamics to restore balance.
Conventional Measures of the Human Biofield Used in Science and Medicine
Some of the field emissions from the body are the basis of many technologies commonly used in clinical diagnosis and research. Thus a significant number of conventional medical tests already provide windows into the human biofield.
Conventional science and medicine have long used the electrocardiogram (ECG) and the electroencephalogram (EEG) to assess physiologic function of heart and brain, respectively. The heart produces coherent contraction of numerous muscle cells, resulting in vigorous electrical activity. In fact, the heart makes the greatest contribution to the electromagnetic, as well as the acoustic, human biofield. The brain’s activity contributes to a lesser extent to the biofield because its field emission is weaker than that of the heart. The ECG was first developed in 1887 and records the electrical activity from different areas of the heart. The EEG was developed in 1875 and records electrical activity from the various brain regions by using multiple electrodes on the head. In addition, corresponding magnetic field measurements of the heart and brain have been discovered, which are the magnetocardiogram (MCG) and the magnetoencephalogram (MEG), respectively. However, the magnetic fields of the body are very low level and typically require specialized equipment such as super-conducting quantum interference devices (SQUIDs) that are expensive to operate. Nonetheless, such magnetic field measurements of the body reveal more information than the electrical measurements, especially if coupled with three-dimensional resolution, as in the case of MEG. For the latter, localizing the activity of a region of the brain approximately the size of a pea is possible. Additionally, some of the more recently developed medical scans, such as functional magnetic resonance imaging and positron emission tomography, can also be used as indirect indicators of electromagnetic activity.
Galvanic skin response (GSR) measures the electrical conductance between two electrodes placed on the skin. This value is a mainstream measure used in lie detectors to help determine veracity and in biofeedback technology to help promote relaxation.
The human body is a strong emitter of infrared radiation, on the order of 100 watts, and visualization of this emission is used in medical imaging. Thermography uses an infrared camera and an associated software system to visualize the pattern of infrared emission, which we cannot see directly but experience as heat. This method can detect changes as small as 0.01° C in the human body. Thermography can detect acute and chronic inflammatory conditions. This method is documented by many research studies to show toxic accumulations, tumors, and other diseases, often much earlier than x-ray mammography or other imaging procedures, for example, in the case of breast thermography (Amalu et al, 2006). Typically, thermography is used to locate hot spots and left-right imbalances that correspond to problem areas. However, the actual temperature and emissions pertaining to the infrared portion of the human biofield have been considered much less important thus far to clinicians and investigators. Thermography is also used before and after therapy to visualize its influence, as for example in the case of infrared photonic treatment to look for improvements in the symmetry of the emission patterns after treatment. Thermography is now an accepted diagnostic procedure in medicine.
In this chapter, no further effort to discuss these conventional measurements will be made. Instead, we will focus on other ways of assessing other components of the human biofield, in particular, such as the energetic systems that may be associated with a subtle life energy or vital force important in self-healing, such as the acupuncture meridian system and the system of the chakras. These methods represent frontier assessment measures and are not yet part of mainstream science or medicine. Nonetheless, they are often of great interest in CAM and integrative medicine.
New Approaches to Measuring the Human Biofield
If a Human Energy Project were to exist to measure all of the electromagnetic components of the human biofield, akin to the Human Genome Project, we would need teams of scientists measuring the emissions at the various frequency bandwidths using a plethora of detectors and measurement devices. This effort would involve measuring different frequency bands within the electromagnetic spectrum emanating from the body ( Figure 20-1 ).
rubik-figure20-01.jpg
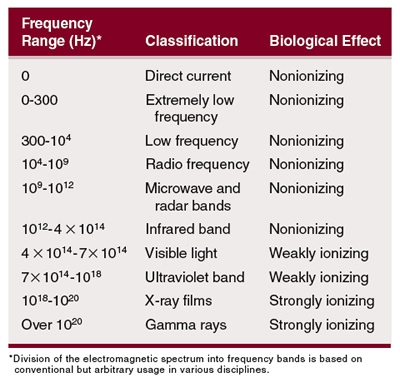
Image provided by Dr. Beverly Rubik
Figure 20-1. The electromagnetic spectrum showing all the known radiant electromagnetic energies.
It includes the full range of nonionizing energies, as well as visible and ultraviolet light, which are ionizing radiation. This spectral range is enormous. In some of these spectral regions, such as the infrared, as mentioned previously, the human body emits relatively high- intensity radiation, whereas in other regions, such as the visible spectrum, the body emits extremely low-intensity light radiation on the order of a few hundred photons per second per square centimeter surface area. Figure 20-2 shows the power spectrum of human emission (Bembenek, 1998).
rubik-figure20-02.jpg
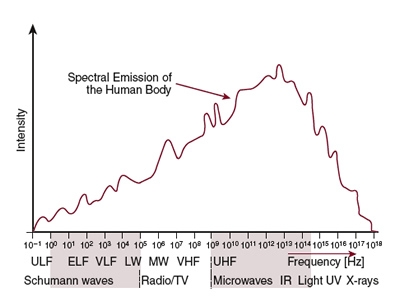
Image provided by Dr. Beverly Rubik
Figure 20-2. The power spectrum of the human body emission.
In foundational research for CAM, more interest has occurred in measuring regions of the human emission spectrum that are unrelated to thermal excitations of biomolecules, as in the case of visible light. Some researchers speculate that the extremely low-level visible light emission from organisms, called biophotons, may be coherent (as in a laser) and may communicate key electromagnetic bioinformation (Chwirot et al, 1987; Popp, 1992, 1998). Some of this research and its possible applications will be described. That such biophoton emission may mediate certain biofield therapies is also possible. Additionally, the induced light emission that is measured as the Kirlian effect from high-voltage electrophotography will also be discussed.
Although we may be able to measure various frequencies of electromagnetic radiation from the human body, these measurements in themselves do not reveal whether the energy is (a) important to life, (b) waste energy, or (c) noise in the system. One way of assessing the components of the biofield that may be central to the living state and especially to healing is to study the therapeutic modalities that apparently employ the practitioner’s biofield: the biofield therapies, such as therapeutic touch, Reiki, Johrei, external qi therapy, and polarity therapy. In most of these modalities, practitioners begin their patient treatment by sensing imbalances in patient biofields and then work to improve their energy regulation by transmitting energy to them, all through the use of their hands. A small but growing body of scientific evidence has been uncovered that biofield therapies show positive physical changes on living systems. In fact, some of the scientific evidence for the biofield and its importance in health and healing comes indirectly from these studies that assess the effects of these biofield therapies on humans and other living systems. More direct evidence of the biofield has been gathered by measuring changes in the practitioner’s or the patient’s biofield before and after biofield therapy or before and after other energy medicine interventions.
We will summarize some of the key findings on biofield therapy that show effects on target systems in the laboratory. These are, in the more literal sense of the term, bioassays, which may help elucidate the key life-stimulating components of the human biofield and the action of these components at the cellular and biochemical levels.
In summary, various strategies for measuring the human biofield include measurements of biophoton emission, as well as induced light emission; measurements on practitioners performing biofield therapy and on patients receiving biofield therapy; and bioassays for biofield therapy, as mentioned previously. Additionally, measurements of the electric or magnetic fields (or both) directly from the human body, especially from the acupuncture points, have also been developed.
Besides the veritable energies of the biofield discussed thus far, the human biofield may also consist of other putative energies as well, more subtle than the energy fields presently known in physics. In relation to this possibility is a less common form of therapy known as distant healing, in which the practitioner and patient are in different locations, ranging from many feet to many miles away. Invoking electromagnetic fields as causal in distant healing is impossible because electromagnetic energies diminish rapidly over distance, varying as the inverse of the square of the distance. Nonetheless, many biofield practitioners, including Reiki and external qi therapists, often learn and practice both local and distant healing. Distant healing, which is often combined with spiritual healing and prayer, may involve no energy transfer whatsoever if it occurs by the principle of quantum nonlocality, or it may involve a putative energy not yet identified in science. However, in this chapter, we will address only specific aspects of the human biofield that are tangible and can be measured. We will also focus only on local biofield therapy.
Devices and Techniques Used to Measure the Biofield
Various devices have been developed that claim to assess aspects of the biofield, most of them electromagnetic in nature. That this area of research is in its infancy, with inadequate funding, no ongoing government sponsorship, and developed by a small number of people working largely in isolation, must be pointed out. Thus, not surprisingly, several issues remain to be resolved.
Here, we describe a few of the devices and techniques that are being used in biofield research or the clinic that appear promising but that need further substantiation to become accepted. These techniques fall into three categories: (1) high-voltage electrophotography, (2) acupuncture point conductivity measurements, (3) and biophoton measurements.
High-Voltage Electrophotography: the Gas Discharge Visualization Camera
The gas discharge visualization (GDV) camera, developed by the Dr. Korotkov Co., St. Petersburg, Russia, is perhaps the best-known form of contemporary high-voltage electrophotography based on the Kirlian effect (Kirlian and Kirlian, 1961) and was first discovered in Russia in 1948. Kirlian photography was not introduced to the West until the 1970s because of communication difficulties during the Cold War. This digital camera, introduced in the West in the late 1990s by its inventor, physicist Dr. Konstantin Korotkov, comes with software and offers the advantage of using a lower voltage than conventional Kirlian photography that is not felt as an electric shock by subjects. A photograph of one of the recent GDV models is shown in Figure 20-3.
rubik-figure20-03.jpg

Image provided by Dr. Beverly Rubik
Figure 20-3. Photograph of the gas discharge visualization (GDV) camera.
Although scientists never widely embraced the Kirlian technique, research was conducted (Boyers and Tiller, 1973; Krippner and Rubin, 1973) and culminated in the founding of the International Kirlian Research Association in the United States in 1976, no longer in existence. Perhaps the most famous experiment is the phantom leaf effect, whereby electrophotography on a segment of a leaf yields a photograph showing the whole (Moss, 1979). Replication of this effect has been achieved but with great difficulty (Korotkov, personal communication, 2002). The Kirlian technique was used clinically in Germany for decades, and the Vega-Grieshaber Company manufactured cameras to record the Kirlian emission of hands and feet. In this setting, energy emission analysis on patients was developed by Peter Mandel, who documented many clinical cases (Mandel, 1986).
The GDV camera uses pulses (10-microsecond) of high-frequency (1024 Hz), high-voltage electricity (10-15 kV) that is selectable from several ranges. The time exposure of the sample is selectable from 0.5 to 30 seconds. In addition to still digital photography, recording digital video is also possible for up to 30 seconds. A charge-coupled detector (CCD), which is a standard detector of low-level visible light used in telescopes and other scientific instruments, detects the pattern of photons emitted from each fingertip. This information is sent by cable to a computer for analysis, as shown in Figure 20-4.
rubik-figure20-04.jpg
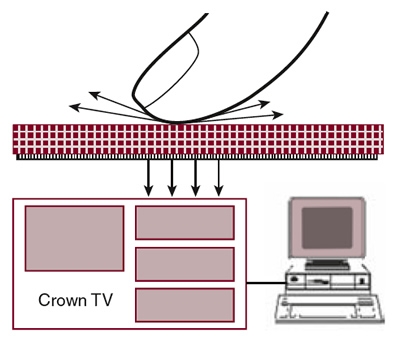
Image provided by Dr. Beverly Rubik
Figure 20-4. Schematic setup of the GDV camera.
The method of use is as follows. The subject sits or stands in front of the camera and is prompted by the researcher to place a given fingertip, one at a time, on the electrified glass plate of the camera, under a lens cover with a special port for the finger, to maintain ambient darkness. The researcher pushes a mouse button attached to both the computer and camera to activate the camera, which sends a pulsed electric field to the plate for the selected time duration. When each fingertip is thus electrified, it emits a corona discharge of light that is then captured by the GDV capture program.
An example of the raw data, a single GDV image from a single finger, is shown in Figure 20-5 . The reader should note that the CCD does not distinguish color; thus the captured GDV images appear black and white.
rubik-figure20-05.jpg

Image provided by Dr. Beverly Rubik
Figure 20-5. GDV photograph of corona discharge from human thumb, raw data.
Theoretical considerations suggest that the GDV images of the fingertips are a complex mixture of a correlate of the biofield plus additional effects. The human subject may be considered as part of a large electrical circuit in the GDV technique. The discharge of light from the finger is the result of a glowing gas plasma of charged particles from the finger to the plate that conducts electricity. This discharge results from a combination of local and global effects from the human subject. Local effects include local skin conductivity and perspiration. The global effects are associated with whole body contributions, including biofield elements such as the acupuncture meridians, which also relate to the common impedance of the body from all the organs and tissues (Figure 20-6).
rubik-figure20-06.jpg
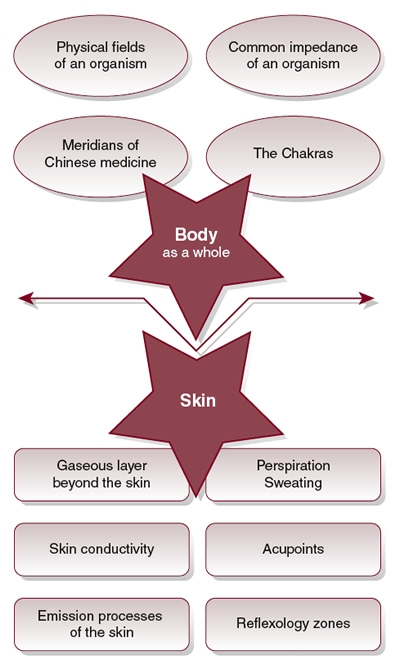
Image provided by Dr. Beverly Rubik
Figure 20-6. Global and local factors in GDV photographs of finger emissions.
The relative contribution of each of these contributing factors to the GDV images for a particular subject is impossible to determine. However, if one uses the GDV camera to make images before and after an intervention and observes the differences between the before and after images, then the geometric effects of local skin conductivity and common impedance remain relatively constant, whereas the perspiration and the whole body contribution correlated with biofield will be the changing factors contributing to any observed differences. Moreover, if one makes GDV images with and without using the GDV filters, which are very thin polyethylene filters that apparently block the effects of perspiration that also contribute to the induced light emission, then one may, in theory, filter out the local perspiration effects and primarily observe the whole-body contribution. An important point to note is that the GDV images are induced light, not natural light, emitted from the body; thus their exact relationship to the natural field of the body, the biofield, are unclear. Nonetheless, meaningful results have been shown in some studies, consistent with improved energy regulation, for example, after qigong, and which are also consistent with measurements from using other types of biofield instrumentation.
rubik-figure20-07.jpg
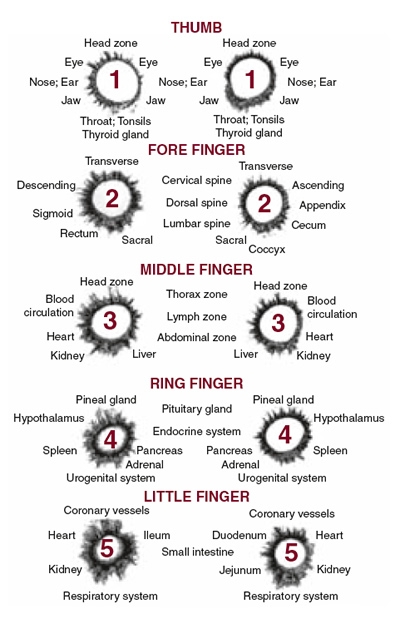
Image provided by Dr. Beverly Rubik
Figure 20-7. Finger emission sector analysis used in GDV software.
Besides the GDV capture program, other GDV software modules have been developed that work in tandem to assess various parameters of the emission patterns, including area, intensity, density, and fractality, as well as details of various sectors of the fingertip patterns that purportedly relate to the bioenergetics of specific organs and organ systems (Figure 20-7) (Korotkov, 2002). A sample organ diagram is shown in Figure 20-8.
rubik-figure20-08.jpg
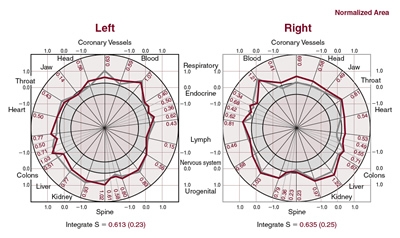
Image provided by Dr. Beverly Rubik
Figure 20-8. Sample organ diagram generated by GDV software, showing the consistency of repeated measurements on different days for a normal person.
The inventor, Konstantin Korotkov, PhD, has reported some standardization of techniques to show the stability and reliability of the GDV parameters (Korotkov, 1999, 2002). Moreover, empirical data showing a correlation between particular sectors of fingertip emissions and diseased organs was published independently by Peter Mandel who studied numerous patients over decades using the older form of Kirlian photography with photographic film (Mandel, 1986). The evaluation of the fingertip sectors and their comparison with particular organs and tissues in the GDV software is said to be based on both the system of acupuncture meridians and su jok (a form of Korean hand acupuncture) (Korotkov, 1999). The assignment of the various fingertip sectors to the seven chakras is offered in a chakra diagram (Figure 20-9) (Korotkov, 2002), but the detailed calculations to define values on the chakra diagram are not reported. A sample chakra diagram is shown in Figure 20-10.
rubik-figure20-09.jpg
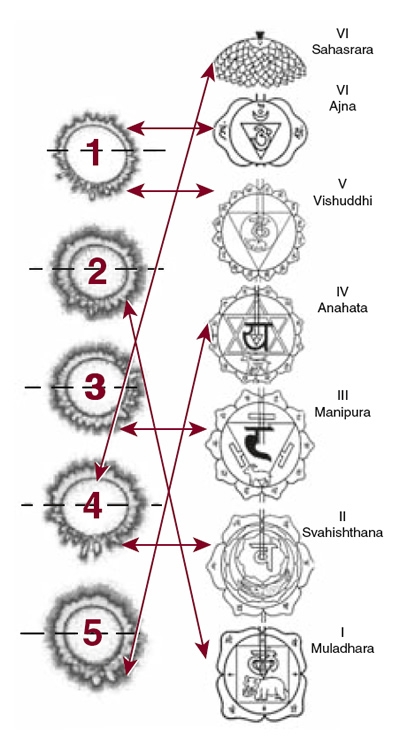
Image provided by Dr. Beverly Rubik
Figure 20-9. Assignment of finger emission sectors to generate chakra diagram in GDV software, in which fingers 1, 2, 3, and so forth refer to the thumb, index finger, middle finger, and so forth.
rubik-figure20-10.jpg
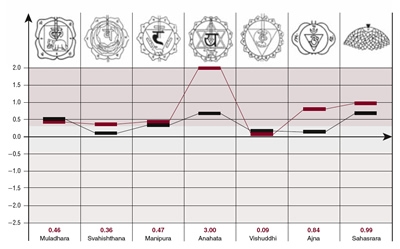
Image provided by Dr. Beverly Rubik
Figure 20-10. Sample chakra diagram generated by GDV software.
The software analyses most useful for researchers, as their algorithms are fully revealed, include the basic parametric calculations derived from the raw data, whereby each finger emission pattern is analyzed for the total and normalized area of illumination, brightness, fractal dimensionality, and density. Each of these parameters is defined by mathematical equations (Korotkov, 2002), thus they have clear objective meaning. An example of a study in which such parametric calculations were made is one exploring how performing qigong influences the GDV images of 16 adult subjects (Rubik and Brooks, 2005). All 10 fingers of each of the adults were assessed using the GDV camera immediately before and after performing Dayan (wild goose) qigong in a group setting. One main observation is that the density parameter increased (p<.01) after qigong, which means that a more uniform circle of light was emitted from the subjects’ fingertips after qigong. Another observation is that the emission patterns from the 10 fingers of each subject showed decreased variability after qigong. These results are consistent with the expectation in oriental medicine that better regulation of qi results from practicing qigong, with qi flowing in a smooth unimpeded manner throughout the body. Although we cannot and may never be able to measure the flow of qi per se, the greater uniformity observed in the GDV images is suggestive of improved energy regulation.
Using a quantum-biophysical model of entropy and information flows and supported by some clinical data, Korotkov, Williams, and Wisneski (2004) advance the concept that the GDV technique provides indirect information about the level of free energy resources (excited electronic states) available in protein complexes in the body. Additionally, Korotkov together with colleagues have published several experimental research papers using the GDV technique in English (and others in Russian) on a wide range of applications to humans, including direct vision (visual perception by means other than through the eyes) (Korotkov et al, 2005), on altered states of consciousness (Bundzen et al, 2002), and in cosmetology (Vainshelboim et al, 2004). Other researchers have proposed the utility of the GDV technique as a holistic medical screening method (Chiang, Wah Khong, and Ghista, 2005).
The GDV technique has been used for clinical studies mainly in Russia (Bevk, Kononenko, and Zrimek, 2000), where it is a registered medical device. It has also been used to monitor the results of stress-management training (Dobson and O’Keffe, 2000). Several studies by other researchers have been performed that explore the usefulness for whole body assessment of human subjects subjects (Rubik, 2002a). Other researchers have used similar high-voltage electrophotographic techniques (not the GDV camera, however) to investigate the reproducibility of assessments of biofield practitioners compared with controls with significant results (Russo et al, 2001). One result observed is that biofield practitioners were able to change their corona discharge parameters by the intent to emit energy, whereas controls were not.
Some words of caution are necessary for future researchers hoping to gather meaningful data using the GDV technique. Careful placement of each finger with light steady pressure on the camera plate is important. Collecting data at the same time of day each day for comparison purposes is also important because of the circadian rhythms in the flow of qi in the meridians. In this way, each human subject can be viewed as having a unique energetic signature in GDV images that is consistent from day to day in adults who are healthy and not receiving therapeutic treatments. New investigators should work to establish this reliability in their data before venturing to conduct studies with the GDV. All devices, including the GDV, provide useful information about the subject in ways that are necessarily limited by the technique, skill, and level of interpretation of the user. Using and interpreting the GDV data requires experience. New users will find that interpreting the results is challenging. In the current state of the art, investigators are on their own in their interpretation of their data, given that no standardized basis for interpreting findings has been established.
Some limitations exist that are specific to the GDV technique. One limitation is that it measures induced light produced by electrifying the person’s finger. The relationship between this induced emission and the extremely low – level natural light of the endogenous biofield is unknown. A second limitation is that, for the human being, the GDV can measure emission only from the fingertips. The software employs various conceptual and mathematical frameworks to apply the data to modeling of energy flow within the tissues, organs, and whole body. Such frameworks include algorithms of oriental medical systems such as the various acupuncture meridian systems and su jok, in which the hand is a homunculus of the whole body. However, the algorithms for these extrapolations from the data are not fully revealed. A third limitation is that the glass plate of the camera will not permit any ultraviolet light in the emission to be detected, given that glass blocks ultraviolet radiation. However, in some cases, for example, in certain altered states of consciousness, the emission patterns become ultraviolet. A fourth limitation, mentioned earlier, is the absence of a large database of human fingertip data correlated with states of health, specific diseases, and so forth; therefore people using this device must use subjective means or develop their own database for data interpretation. A documented database and device standardization needs to be published in peer-reviewed journals to make that the GDV camera is a truly scientific instrument. A fifth problem for research is the many different models of the GDV camera, without any attention to model numbers or the manufacturer revealing the differences between the models. Researchers who possess more than a single version of these devices have noted differences in results obtained with the various models. Therefore a lack of standardization appears to exist.
No reliability studies have been published on the use of the GDV camera. However, one study on reliability on a related technique showed moderate reliability (Treugut et al, 1998).
In conclusion, the GDV and related techniques appear to be able to measure certain aspects of biologically generated electromagnetic fields contained within the corona discharge that are relevant for CAM. However, a concerted effort is needed to delineate and resolve the various issues described previously so as to advance the use of this method for biofield science.
Acupuncture Point Conductivity Measurements
A considerable number of devices are available today that use a method of assessing electrical conductivity of the skin through the acupuncture meridian system for the purpose of providing information about the energy flow related to the health of the body. This technique is known by various names, including electrodermal screening (EDS), electrodermal testing (EDT), and electroacupuncture according to Voll (EAV). In the United States, many of these electrodermal devices have been categorized by the U.S. Food and Drug Administration as biofeedback devices for meridian stress and more recently referred to as devices for meridian stress assessment (MSA) and living systems information biofeedback (LSIB). Just as electrical conductivity measurements provide biofeedback on a patient’s nervous state to practitioners using GSR, EDS devices provide direct biofeedback or information on the biofield status or response of the patient. One main use for these devices in the West is allergy testing, although they are used for a variety of other purposes as well, including oriental medicine evaluation. Various corporations market these devices, including Vega, Biomeridian, and Health Epoch, to name a few.
In 1950, Reinhold Voll, a German physician, was studying the acupuncture meridian system. He reasoned that if acupuncture points were portals on the skin for channels of qi running through the body, then measuring this energy at the acupuncture points should be possible. Voll constructed a device to locate the acupuncture points by virtue of their greater electrical conductivity compared with the surrounding skin. He found correlations between disease states and changes in the electrical properties of the various acupuncture meridian points (Voll, 1975). Furthermore, Voll made two discoveries:
1. Indicator drop. Voll compared the acupuncture point measurements of healthy patients with those of patients who had conventionally diagnosed diseases. He found that the electrical conductivity of healthy acupuncture points measured were within a given normal range, whereas readings outside of this range revealed disturbances in the tissues and organs sometimes associated with these points. In addition, Voll noticed that major disturbances in the body produced a downward drop, or steady decay, of the conductivity indicator as the point was being measured. This effect became known as the indicator drop (Voll, 1975).
2. Medication test. Voll discovered by chance that closed bottles of medicines placed in the proximity of the patient could change acupuncture point conductivity values (Voll, 1977). This test became known as the medication test. Such testing may provide useful diagnostic or therapeutic information. Apparently, substances such as homeopathics in the vicinity of the human subject may alter the subject’s biofield by means of a resonance phenomenon. However, no consensus has been reached on the modus operandi for such an effect.
Many case reports documenting the success of EDS have been published. In addition, a few published studies have documented physiologic correlates or patient outcome (or both) for certain medical applications of EDS. Sullivan and colleagues at the University of California Los Angeles reported that patients with lung disease confirmed by x-ray examination had 30% lower electrical conductivity readings taken at acupuncture lung points than those of healthy patients. An 87% correlation was found between the testing results for the lung points and the x-ray testing for lung cancer, whereas no correlation was found for small intestine acupuncture points (Sullivan et al, 1985). Lam and Tsuei at the University of Hawaii have published approximately two dozen papers establishing the correspondence of EAV readings with physiologic disturbances. In one study, the authors showed that in the treatment of diabetes, EDS was a beneficial adjunct to the conventional diagnostics in determining the proper allopathic doses of insulin and glyburide, as well as homeopathic remedies and nosodes (Lam, Tsuei, and Zhao, 1990). In a double-blind study on allergy testing, six different diagnostic methods for allergy testing were compared—history, food challenge, skin testing, radioallergosorbent test, immunoglobulin E antibodies, and EDS—on 30 subjects. In over 300 tests, EDS matched the history 74% of the time and was most compatible with the food challenge test, which is considered to be the most sensitive of all tests for food allergy (Tsuei et al, 1984). Use of EDS is greater outside the United States, and much of the literature on it has been published in German, French, Japanese, and Chinese.
Many different types of EDS devices and associated measurement techniques have been developed. However, two main schools of EDS have been established, which we refer to here as the Western and Eastern schools.
The Western school evolved in Germany through three main phases: EAV, bioelectronic functions diagnosis (BFD), and the VEGA resonance test (VRT) (Rademacher and Wesener, 1999). The first commercially produced EAV instrument in Germany was the Dermatron, manufactured by Pitterling Electronics GmbH in 1956. EAV was a laborious procedure that involved testing hundreds of points on a person. BFD simplified the EAV procedure; it introduced silver electrodes that conduct electricity better than the brass used in EAV, it introduced a sector measurement to assess any blockages in regions of the body, and it used only a few dozen acupuncture points on the hands and feet. BFD practitioners soon discovered that a single acupuncture point could be used for all testing, which made the procedure much faster and easier to use. This discovery led to the VRT and a new device designed in 1978 by Helmut Schimmel, MD, DDS, together with VRT. The Western style EDS devices are tools that can access aspects of the body’s biofield control system and communicate with it to obtain answers about the patient’s sensitivity to and need for nutritionals, remedies, and environmental substances. By these means, EDS may help diagnose conditions and diseases because it provides a highly individualized way to pose questions of the patient’s condition and obtain answers at the energetic level.
In contrast, the Eastern school of EDS devices draw on Ryodaraku theory from traditional oriental medicine. This theory was developed by Yoshio Nakatani in Japan in 1949. It is based on the principle that disease is thought to be reflected by the 12 source acupuncture points (Oda, 1989). If excess energy is being conducted at a given point, it is called excitation (fullness), and if a lack of energy exists, then it is called inhibition (emptiness). This discrepancy or inconsistency among the meridians that indicates excess excitation and inhibition causes illness. Nakatani also discovered age, gender, and seasonal variations in the conductivity values and that when the values are generally higher, the subject’s autonomic nervous system is hyperaroused.
The Voll and Ryodoraku methods use almost the same technique of checking the indicator drop conductivity value of each acupuncture point. However, the two schools typically measure different points. Normally, the Voll school measures some 40 points that are different from the 24 points measured in Ryodoraku. Moreover, the Voll method is more organ based than meridian based. The Voll method uses measurements at acupuncture points for bioinformational purposes and has narrowed its focus down to a small number of these points using a distinctly Western orientation to health and disease, including use of homeopathy in many of the test remedies. By contrast, the Ryodoraku method assesses meridian stress according to oriental medicine principles. For example, in Chinese medicine, an abnormal liver meridian does not necessarily mean that the liver organ itself is abnormal; rather, it refers to a primary energetic imbalance.
One quality device that is based on the Ryodoraku method is the Electro-Meridian Assessment System (EMAS). No training in acupuncture is required to use this system. The device is easy to learn and operate even for beginners. Made by Health Epoch, Inc., the EMAS is composed of a portable measuring device and application software. The electrical conductivity of the 12 source acupuncture points of the body, on the left and right side, is measured, and the resulting values are analyzed by the software package in multiple ways according to the different schools of oriental medicine.
rubik-figure20-11.jpg

Image provided by Dr. Beverly Rubik
Figure 20-11. Schematic setup of the Electro-Meridian Assessment System (EMAS).
The EMAS device is essentially a computer card housed in a metal casing that connects to a computer universal serial bus port and an alternating current (AC) power outlet (Figure 20-11).
The probe, which is attached to the device via electrical cables, is a 1-cm round, hollow metal, spring-loaded device with a plastic handle. In addition, the patient holds a grounding rod in the opposite hand during measurement (Figure 20-12).
rubik-figure20-12.jpg

Image provided by Dr. Beverly Rubik
Figure 20-12. Photograph showing subject undergoing measurement using the EMAS.
The constant-pressure probe ensures measurement stability and is fitted with a ball of cotton saturated with saline solution for optimal conduction. A simple automatic calibration is performed to ensure the accuracy of the EMAS system just before measuring a subject. When properly calibrated, the maximal current entering the subject’s body is 200 microamperes, for which 95% of subjects experience no sensation during measurement. The practitioner is then prompted by the software precisely where to position the probe on the subject’s body for each point measurement in a sequence from the left to the right hand and then from the left to the right foot. The practitioner manually holds the probe in place while the electrical conductivity is assessed at each point. The measurement of all the points takes approximately 5 minutes. After the final measurements are obtained and the data are saved, the software immediately displays the resulting bar chart of meridian conductivities (Figure 20-13).
rubik-figure20-13.jpg
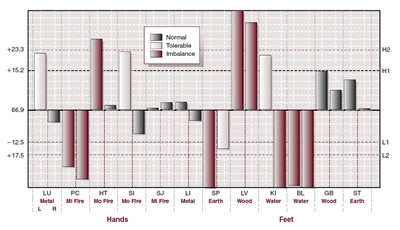
Image provided by Dr. Beverly Rubik
Figure 20-13. Example of the bar chart showing the 24 acupuncture point conductivity values generated by EMAS software.
Normal values are shown with green bars, tolerable values in yellow, and abnormal readings in red bars. At a glance, the practitioner can note which meridians are unbalanced. Other analyses of the data can be made, depicted on subsequent screens in the software (not shown here), including the average body energy or overall qi, the upper and lower body energy ratio (hands vs. feet), the left and right side energy ratio, the internal (yin) and external (yang) energy ratio, and the autonomic nerve ratio. The software produces a report showing the results for a given patient, which also suggests different types of treatment, including different styles of acupuncture, acupressure, aromatherapy, Chinese herbs, dietary recommendations, and more. Although the EMAS is primarily designed for clinical practice, it can also serve as a useful tool for research in biofield science. It is particular well suited for investigating the before and after effects of any intervention on the acupuncture meridian system; it also provides a detailed view of the human energy system from the perspective of several different oriental medicine systems, which is unique. A small number of studies using the Ryodoraku method have been published in English (Sancier, 2003; Schmidt et al, 2002).
In summary, all EDS machines measure the body’s electrical conductivity. Although different electrode specifications and measurement parameters may be used by various manufacturers, the goal is the same—to assess the health of the body through its ability to conduct microcurrent. Simply stated, healthy bodies conduct microcurrent more readily and more uniformly than unhealthy ones.
Many advantages have been discovered to using EDS over other evaluation methods, such as its speed of use, individualized approach to care, and the fact that it is inexpensive relative to conventional biomedical testing. However, new users of the Western-type EDS may find that training by qualified teachers, as well as considerable time to learn and to practice on their own until they feel confident to use it clinically, is required, although the newer devices are easier to use than the older ones. The practitioner must learn how to manipulate the probe and how to find the acupuncture points and in what sequence to do the testing. Many practitioners who learn this technique find that it can transform their practice in that they have consistent, positive results with patients and come to rely on it. EDS is particularly useful for functional medicine—a type of CAM in which individualized assessment and early intervention are used to improve physical, mental, and emotional function. Such is the case in both the Eastern and the Western methods.
Research is needed to gain understanding of the significance and interpretations of EDS measurements of conductivity and, more fundamentally, of the responsiveness and possible causal role of the acupuncture meridian system in relation to health status. Most importantly, nobody fully understands how dysfunction or disease correlates with the electrical conductivity of certain points on the skin in a consistent way, although this correlation has been empirically observed by many researchers and clinicians worldwide. More basic research in this area, plus further studies that would extend the validation of the EDS, is recommended
The accuracy of EDS measurements may be somewhat dependent on the practitioner’s skill and technique, as associated, for example, with calibrating the instrument, placing the probe properly on the acupuncture point, maintaining consistent pressure with the probe, avoiding physical contact with the patient except at the measurement point to minimize energetic interactions, and the consistency of procedure throughout the measurement process. New probes should be studied to evaluate their precision, reliability, and operator dependence relative to older probes. Further reliability studies are also needed for this technology, especially given that electrical stimulation at the acupuncture points associated with measurements may alter the bioenergetics of the body, possibly jeopardizing the consistency of repeated measurements over short periods.
A main obstacle to the acceptance of EDS is an attitude on the part of the conventional medical community that has historical origins. Back in the 1800s, the use of electricity in medicine was widespread. Around 1900, a large number of medical practices came into question, and the Carnegie Foundation established a commission headed by Abraham Flexner to investigate. The report, published in 1910, became widely known as the Flexner Report and produced widespread changes in medical practice and medical education. Electrotherapy disappeared from medicine and became regarded as quackery. Nearly a century later, in an age of pharmaceutical dominance, the medical community is still largely suspicious about EDS, despite the growing use of this modality in CAM.
Biophoton Measurements
A substantial body of research exists on ultra-weak light emission from various organisms (Cohen and Popp, 1997; Devaraj, Usa, and Inaba, 1997), including humans (Van Wijk and Van Wijk, 2005). This type of energy is extremely low level, but it can today be accurately measured with sophisticated instrumentation that is generally customized (Lin et al, 2006; Van Wijk and Van Wijk, 2005). Systematic measurements of this extremely weak light emission from the body, the waveband of which is in the visible range from 400 to 720 nm in wavelength, represent one approach to assessing the radiant nonthermal human biofield. This range might be correlated, as expected, to changes in health, disease, healing, and altered states of consciousness, according to the biofield hypothesis.
The investigation of light emission from organisms began with discoveries of Gurvich (1874-1954) who noted that mitosis was stimulated in regions of onion roots exposed to one another through a quartz barrier by what he proposed to be mitogenetic radiation. He also identified secondary emission, by which regions of the organism receiving mitogenetic radiation emit light, and a third phenomenon, known as the degradation effect, which refers to the burst of light released when living organisms are damaged or exposed to toxins (Gurvich, 1959). Gurvich also postulated the morphogenetic field theory of life (Lipkind, 1987), a precursor to Sheldrake’s (1981) morphogenetic field concept and the modern biofield hypothesis (Rubik, 2002 ). He regarded the biologic radiations that he investigated as support for his theory of a deeper collective order in the regulation of the organism.
Research in this area advanced when low-level light detection technology improved in the 1950s and 1960s such that the ultra-weak emission from organisms, which ranges from a few to hundreds of photons per second per square centimeter of tissue could, in fact, be measured. Early systematic measurements of human biophotons attempted to record the radiation from naked subjects with photomultiplier tubes and found that the noise in the detector was approximately the same order of magnitude as the signal. Nonetheless, researchers were able to integrate the signal over time and then found it to be statistically significant over the noise. In related experiments, subjects were actually asked to increase their light emission, and an increase in the signal was found to be significant over controls (Dobrin et al, 1975, 1979). Using coolant ( – 23° C) to reduce the noise of the photomultiplier detector, Edwards and colleagues (1989, 1990) counted photons over time from body regions. The authors found that the abdomen, lower back, and chest emitted from 4 to 7 photons per second, whereas emission from the forehead and hand were larger, on the order of approximately 20 photons per second. Furthermore, if a tourniquet were tied around the upper arm, the photon emission of that palm of the hand was reduced 15%.
Three types of systems are presently used to measure biophotons: (1) photomultiplier tubes, cooled down to minimize their noise, which register photon counts over time; (2) a spectral analysis system, using a set of cut-off optical filters to determine the wavelength characteristics of the emitted light; (3) and a two-dimensional system of sensitive photon-counting devices, including arrays of cooled photomultipliers and CCDs that produce biophoton images (Van Wijk and Van Wijk, 2005).
In 1993, Popp and colleagues in Germany created a special darkroom with a cooled photomultiplier that could be moved around to scan the whole body of a subject lying on a bed below. Two hundred persons were measured. The results show that biophoton emission reflects (1) the left-right symmetry of the human body; (2) biologic rhythms such as 14 days, 1 month, 3 months, and 9 months; (3) disease states reflected in the broken symmetry between the left and right side of the body; and (4) light channels in the body, which are hypothesized to regulate energy and information transfer between different parts of the body. One main aim of Popp’s continuing human studies is to identify specific regions of the body, the emission characteristics of which might differentiate states of health and disease in an integral way (Cohen and Popp, 1997, 2003).
The relationship of biophoton emission to oriental medicine has been investigated through several studies. In one study done in Korea, biophoton emission counts from the dorsal and ventral sides of the hands of three healthy human subjects were measured for 52 weeks. Results show that the emission rates were lowest in autumn. Although the emission rates from the palms remain rather stable throughout the year, those from the dorsa vary widely, depending on the season (Jung et al, 2005). In another Korean study, left-right biophoton asymmetry from the hands of seven patients with hemiparesis was studied. Findings revealed that the patients with left hemiparesis emit more biophotons from the right than from the left hands, whereas the opposite was found for the patients with right hemiparesis. Acupuncture treatment dramatically reduced the left-right asymmetry of biophoton emission (Jung et al, 2003). Another study showed that significantly more emission was recorded from the fingernails than the fingerprints for each subject’s fingers (Kim et al, 2002). Still other studies suggest that the biophoton emission from the acupuncture points is generally higher than that of the surrounding skin (Inaba, 2000). Moreover, needling or using other means of stimulating the acupuncture point enhances the emission over that of other acupuncture points (Inaba, 1998). Inaba also used a system of two-dimensional photomultipliers to record the two-dimensional pattern of biophotons from the surface of the hands. He showed that the index and middle fingers of a subject had the highest intensity (Usa et al, 1991). Interestingly, these two fingers are considered the sword fingers in certain styles of qigong and are sometimes considered to be the chief emitting fingers in giving external qi.
The biophoton emission from humans in studies on consciousness has also been investigated. In eight subjects, Vekaria (2003) investigated the influence of intention to change one’s emission on the measured biophoton emission and found that the mean photon count decreased, but not all subjects were able to achieve this change. Measurements made from the hands and foreheads of five meditators showed that biophoton emission decreased after meditation (Van Wijk and Ackerman; Van Wijk, 2005). Another study of transcendental meditation (TM) subjects in particular showed that regular meditators have the lowest biophoton counts and that biophoton emissions of meditators and controls did not vary much in anatomic distribution, except for the throat and the palm of the hand (Van Wijk et al, 2006). Because free-radical reactions are thought to be responsible, at least in part, for the biophoton emission, the results also suggest that TM helps reduce free-radical reactions in the body.
Two schools of interpretation of biophoton emission exist that reflect the age-old struggle between vitalism and mechanism. One school is the chemiluminescence school, which holds that the ultra-weak emission from life can be understood solely in terms of known principles of chemiluminescence from free radicals as a byproduct of cellular chemistry and that such light emitted is from random processes and thus carries no signal. The other school, which we term here the biophysical school, retains the Gurvich heritage and maintains that the organism is a radiator and antenna of a particular range of electromagnetic frequencies or biophotons that are coherent (in phase) and are used for communication, growth, and regulation in the living state. Long-range coherent interactions in living systems are also expected from other physical considerations (Frohlich, 1968). Liboff (2004) also wrote of the electromagnetic unity of the organism. Several researchers have hypothesized that the electromagnetic field emission from the human body is, at least in part, coherent and can carry information that is involved in organizing biomolecular processes (Inyushin, 1978; Popp, 1998; Rubik, 2002b ). Photon-count statistics on the distribution of photons in the emission should provide an answer to this question (Kobayashi, Devaraj, and Inaba, 1998; Van Wijk and Van Wijk, 2005). Possibly, both schools of interpretation are only partly correct because the biophoton emission may be a mixture of signal amidst some noise of free radical luminescence.
Over the decades of research in this area, several studies have made progress in investigating human biophoton emission in both basic and applied research. Some recent results suggest the rudiments of a new powerful tool of noninvasive medical evaluation on the horizon that will monitor biophoton emissions to assess basic regulatory functions of the human body. Nonetheless, only a limited number of studies has been conducted investigating a very limited number of human subjects in these studies, making any firm conclusions premature. In addition, substantial difficulties exist in making reliable measurements of such extremely low – level light; thus more development of measurement technologies will be necessary before systematic studies can be pursued.
The handling of subjects is also problematic for these studies. Collecting the spatial data on humans is difficult, which requires that they remain still for a long time, with the risk that their blood flow may decrease in the process, affecting the biofield that researchers hope to measure. This risk has been demonstrated by the tourniquet experiment mentioned previously, which showed the importance of blood flow to biophoton emission. Moreover, studies also show the importance of subjects’ states of consciousness, which should also be analyzed along with biophysical and physiologic correlates of photon measurements.
Toward New Assays for the Human Biofield: Basic Research on Biofield Therapies
The various biofield therapies may involve key changes in the human biofield and the transmission of energy field components that are especially important for healing. The biofield therapies include external qigong therapy, therapeutic touch, Reiki, Johrei, pranic healing, polarity therapy, and other modalities. Typically, the practitioner uses his or her hands to sense a deficiency or imbalance in the patient’s biofield and then proceeds to alter or influence this imbalance by means of a subtle energy. The various biofield practices coevolved with different ideas about the origin of the energy transmitted and the role of the practitioner. In external qi therapy and polarity therapy, the energy is thought to move from the practitioner’s body to the patient. In Reiki, Johrei, and therapeutic touch, the energy is considered to come from universal source (the cosmos, divinity, and so forth) to patient, guided by the practitioner, who is viewed only as a conduit.
Studies on these biofield therapies in themselves may offer clues to certain key components of the human biofield that are associated with healing. A key study by Syldona and Rein (1999) suggests that the direct current (DC) potential of the acupuncture meridian system is a key component in the flow of qi in the body and is discussed later. An important factor to keep in mind is that these studies may show either the effects of an energy field associated with the human biofield of the practitioners or the effects of a universal life energy source on which they may draw, or some combination of both. Also possible is that the living targets of these biofield therapies may respond more to putative energies that are not measured by laboratory instruments.
Published studies demonstrate some definite effects from biofield therapies on various target instruments or living systems in the laboratory. Most of these studies have been in pilot studies with small numbers of practitioners as the human subjects. However, with few exceptions, the studies have shown small effects in magnitude and rather high variability. When practitioners trained in the same biofield therapy are studied in the laboratory, a great deal of variability results in their effects on target instruments, organisms, or humans. In addition, difficulty has been found in reproducing results with the same practitioner over time. The source of this variability is not well understood, but one hypothesis is that it may be the result of differences in mood or physiologic states of the practitioners (Rubik et al, 2006 ). That the different levels and range of experience of the practitioners may also contribute significantly to the variability of results is also possible. Although Reiki offers a certification program, many other practices do not have any standardization. This lack of standardization causes further difficulties for research on biofield therapies.
These findings from basic research, if replicated by others and further developed and standardized as tests, may also prove useful as assays or bioassays to measure the level of bioinformational energy delivered by human hands. In this way, we may learn more about the healing modes of the human biofield and how it interacts with the cellular and biomolecular levels of order. Ideally, researchers should have more objective standards for calibrating the healing power of a biofield practitioner. Some recent studies on biofield therapies are discussed briefly he re.
External Qi
A body of literature has been published on the effects of external qi transmitted by qigong therapy practitioners on living systems in vitro, including effects on cell cultures and biomolecules. However, some of these studies lack critical controls, involve only a single qi-emitting practitioner, or use outdated technologies. Nonetheless, some recent improvements have occurred in the quality of research in this area. One key example is a study done at the Walter Reed Research Institute that used a fluorescent probe to measure changes in intracellular free calcium concentration associated with emission of external qi, which is apparently the result of changes in cell membrane channels (Kiang, Ives, and Jonas, 2005). Another example is a study conducted at a university in Taiwan, showing that exposure to external qi significantly decreased the growth rate of prostate cancer cell cultures as compared with untreated cell cultures (Yu, Tsai, and Huang, 2003). Moreover, the authors showed that the treated cells showed increased differentiation, as indicated by the expression of a tissue-specific enzyme. A third example is a study conducted in academic laboratories in both China and the United States, indicating that external qi caused a small change in the circular dichroism spectrum of poly D-glutamic acid, which may reflect a change in the secondary structure of the polypeptide (Chu et al, 2001). These studies use some of the latest biomolecular techniques with high specificity to show how external qi may interact and cause changes in living systems.
A series of studies on the effect of external qi therapy on cultured brain cells was conducted in China (Yount et al, 2004). Proliferation of normal cells in culture was quantified as colony-forming efficiency (CFE). In a pilot study with eight experiments, results show a trend toward increased cell proliferation in the samples treated by external qigong therapy (qigong/sham CFE ratio > 1.0). A statistically significant trend of increased proliferation after qigong treatment was also found in a subsequent study with 28 experiments. However, in a further study with 60 experiments to replicate the previous studies, results showed a nonsignificant but slight increase in proliferation after external qi treatment. When the results from all three studies were pooled to form summary statistics, including an overall t-test for significance, the mean for the qigong/sham data was above 1.0 but not statistically significant (Yount et al, 2004).
Measurements of DC potentials on the skin of qigong healers was made for different states of being, including external focus, healing at a distance (external qi), and self-healing (internal qigong) (Syldona and Rein, 1999). The authors found a statistically significant difference between the rate of changes in the values of electrodermal measurements on and off acupuncture points and between external focus and healing states. They also found that subjects’ self-reported sense of the internal flow of qi correlated with DC potential readings but only for specific measurements made on acupuncture points. Their results showed no clear distinction between external and internal qigong. These findings support the hypothesis that the patterns in the temporal fluctuations of the DC electrodermal acupuncture measurements correspond to the traditional Eastern concept of qi circulating in the body.
Therapeutic Touch
Evidence was found of shifts in the magnetic field emitted by practitioners performing therapeutic touch, as measured by a SQUID magnetometer (Seto, et al, 1992). In a subsequent study, the biomagnetic component of a therapeutic touch practitioner showed a field with a variable frequency around 8 to 10 Hz (Zimmerman, 1989). These studies suggest that the 8- to 10-Hz frequency band may be associated with emission from the human biofield during this therapeutic intervention. Interestingly, this frequency band is also the alpha rhythm of the brain during relaxation and part of the natural resonance frequency bandwidth of the earth, known as the Schumann resonance.
Another study investigated the effects of therapeutic touch on bone cells in culture (Jhaveri et al, 2004). It significantly stimulated primary human osteoblast proliferation, matrix synthesis, and mineralization compared with controls. Other studies with human osteoblasts revealed that therapeutic touch stimulated normal human osteoblast adhesion, with significant changes in integrin levels. Additional work has shown a significant increase in fibroblast, osteoblast, and tenocyte proliferation with therapeutic touch treatment, with different dose-response curves to therapeutic touch dependent on cell type. These data were confirmed by immunocytochemistry.
Reiki
A portable three-axis digital gaussmeter, which can detect milligauss levels of magnetic fields (AC and DC), was used to monitor Reiki practitioners (n = 17) and healers from several different healing traditions ( n = 15) who were instructed to transmit biofield therapy. Highly significant increases in extremely low – frequency (ELF) fluctuations were observed compared with baseline controls and were observed for both hands of practitioners. Moreover, significantly larger increases in ELF fluctuations were observed with more experienced practitioners. Thus changes in ELF magnetic fields were correlated with the practitioner’s sense of biofield manipulation (Connor and Schwartz, 2007). In a separate study that attempted to develop a literal bioassay for biofield therapy (using organisms as the measuring instrument), Reiki treatments on the growth of bacterial cultures (Escherichia coli K12) that had been damaged by heat shock treatment were analyzed along with a determination of the influence of healing context and practitioner well being on such effects. In the healing context, the Reiki-treated plates exhibited an average of 2.6% more colonies than controls in 59% of the trials. Practitioners’ social and emotional well being correlated with bacterial growth in both the healing and the nonhealing contexts (Rubik et al, 2006).
Pranic Healing
Dr. Joie Jones conducted studies on the effects of pranic healing on cultured cells at the University of California, Irvine, over many years (Jones, 2001). Using a bioassay with HeLa cells (a cell line derived from cervical cancer cells taken from Henrietta Lacks, who died from her cancer in 1951) in culture subjected to gamma radiation, the radiation survival rates for the cells with and without pranic healing were determined. To date, 520 experiments have been conducted of 10 culture dishes each involving 10 different pranic healers. Results from 458 of the experiments indicated that treatment of the cells with pranic healing produced a dramatic increase in cell survival rate, from approximately 50% in control cells to approximately 90% in treated cells. In 62 experiments, however, the healer produced no effect whatsoever. Jones noted that a subtle energetic conditioning of his laboratory contributed by the practitioners led to a stronger beneficial effect from pranic healing. Collectively, these experiments suggest that the condition of the energy environment in which studies are conducted may contribute to the variability of responses (Jones, 2006).
Some Key Issues — Complications in Validating Biofield Measurements But a New Dimension in Prognosis
Some anticipated complications have been discovered in seeking correlations between biofield measurements and conventional physical diagnoses. One problem is that biofield measurements assess energetic aspects of the body, which may either precede physical changes or possibly correlate with the present physical status of the body. Thus one may observe putative false positives in biofield indicators that actually reflect a pathologic process that has not yet developed in a measurable disease state or physiologic condition. This factor is in concordance with the principle of oriental medicine that blood follows qi; that is, the physical body will change according to the present status of the biofield. Second, one may also observe false positives (that is, failure to correlate with conventional diagnoses) for minor problems, particularly transient ones, of which the patient may be only minimally aware, or for conditions that may be subclinical or not yet fully resolved. Nonetheless, various biofield measures, such as the MSA, are believed to have predictive value for the appearance of disorders and diseases before they physically develop, allowing preventive action to be taken. The situation is similar to the status of certain conventional biomedical markers, such as blood levels of C- reactive protein, which may appear elevated during the course of a cold as a result of a virus, as well as a serious chronic degenerative disease such as cancer. Third, certain aspects exist to the biofield that may fluctuate rapidly such that no reliability in measurement may be seen, which may be the case for certain subjects more than others. Repeated measurements may yield different values because the subject’s energy may be rapidly shifting. Such variability may be expected in subjects with poor energy regulation.
Interpreting any single clinical finding without observing a constellation of evidence is generally inappropriate, which, taken together in a clinical context, points to a definitive result. In any case, we anticipate that biofield measurements may not be definitive but will add yet another dimension to the clinical picture and the resolution of the health problems of a patient.
Because of these various complications, biofield measurements, in themselves, may never screen or diagnose populations reliably for disorders and diseases. Nonetheless, comparing biofield measurements of a specific subject over time may show meaningful changes that relate to the person’s state of health and may even provide evidence of a developing pathologic abnormality. The latter is known as an ideographic approach in the field of psychology. Such a method is applied in medical thermography, for example, to assess for changes in breast thermograms over time that may reflect a developing cancer. Thus an ideographic approach may be a more useful method in biofield science than the conventional scientific nomothetic approach, which is the quest for lawlike regularities in the study of large numbers of subjects. In CAM, which uses many individualized, as well as multiple, therapies to treat conditions and diseases, the ideographic approach may, in fact, be the only meaningful method.
The possibility also exists that the biofield will shift because of transient thoughts or feelings of the patient. In relation to this phenomenon, certain patients under medical examination exhibit white coat hypertension that yields a false-positive result for hypertension. Can we see a relationship between the transient shifts in biofield parameters and shifts in consciousness of the patient? Should we be investigating this spectrum, which may represent the dynamical mind-body spectrum for the patient?
Another possibility is that the biofield of some patients will shift with the thoughts, intent, or feelings of their practitioners. Findings suggest resonance effects occur in therapeutic partnerships between patient and practitioner (Caldwell-Bair, 2006).
On the other hand, an advantage can be found to observing indicators of the future state of the patient energetically using biofield measurements. That is, by the principle of oriental medicine that blood follows qi, positive changes observed in the biofield after a medical intervention may be expected to correlate with a therapeutic benefit from that intervention. In this way, biofield measurements may be useful prognostically, as well as diagnostically.
The primacy of the biofield over the material body, a belief held by many people since ancient times, means that the material aspect of the body is subordinate to the energetic and not the reverse. All disease may show first via imbalances in the biofield. Self-healing involves changing the biofield, which then organizes changes in the tissues at the deepest levels of the biochemistry. This concept is a radical departure from the conventional biomedical view that holds biochemistry to be the prime mover.
Conclusions and Prospects for the Future
An overview of biofield science with respect to human biofield measurement and application to CAM was provided in this chapter. A growing body of basic science data can be found, preliminary and pilot studies, that provide support for the concept of a biofield. Further theoretical and experimental research is needed to refine and standardize the measurements of the biofield, develop new techniques, explore its relevance to health, disease, and healing, and otherwise continue to explore this frontier area. Three categories of biofield measurement from humans have been reviewed: (1) high-voltage electrophotography, (2) EDT, and (3) natural light emission (biophotons). EDT is more clinically useful than the other methods, whereas the GDV camera and biophoton measurements are largely still tools for exploration in basic and clinical research, with fewer clinical applications.
Indeed, the data taken collectively from these explorations reveal that the human biofield is as a flickering flame of energy: dynamic, with some coherence and stability and with some elements of chaos and unpredictability.
The lack of validated measurement tools and energy markers remains an obstacle to progress in biofield science and medicine. The peer-reviewed literature, at least in English, reveals no biofield instruments to date that have been well documented or generally approved by the research community. No substantial database of conditions and diseases correlated with any energy field measures of the human body has been published. Reliability and validation studies are scarce. No device has been consistently shown in controlled trials to produce energy field measurements that correlate well with diagnoses or therapeutic effects. Moreover, some of the commercial devices for measuring biofield components have algorithms for data analysis or interpretation that remain obscure or only vaguely revealed. Thus, in many cases, the parameters derived from raw data via the software and their significance are unclear. More work is needed to bring the technology into greater acceptance for both research studies and the clinic.
A large influx of funding for biofield science is recommended to support a concerted effort over the long term by a larger community of collaborating scientists. Work in isolation by only a handful of researchers is insufficient to bring this work to full fruition.
Besides refining the techniques, future research approaches should include, but not be limited to, the physical characterization of the biofield, examination of mechanisms down to the cellular and molecular level for sensing and studying the emissions of the biofield, and the influence of psycho-logic and physical states on these processes.
The study of the mutual coupling of fields and radiative emissions on the one hand with biomolecular processes on the other, or otherwise stated, the intersection of biofield science with biochemistry, is a key research challenge for the future. Once we clearly identify the various modes of this coupling, our understanding of energy medicine and other CAM therapies, and indeed of life itself, will move to a new level.
Also at the cutting edge of biofield research is the question of how the biofield may shift as a result of shifts in consciousness. Understanding more about the human biofield in connection with psychophysiologic states such as healing and altered states might help facilitate an understanding of mind-body regulation and help build a bridge between energy medicine and mind-body medicine.
Acknowledgments
The author gratefully acknowledges the helpful input and assistance from Dr. Spencer Huang; Terrance Pan, LAc; Dr. Larry P. Goldberg; and Dr. Roeland van Wijk.
For more information, contact Dr. Beverly Rubik; Lab phone: 510-428-4084.
References
Amalu et al: Infrared imaging of the breast—an overview. In Bronzino J D, editor: The biomedical engineering handbook, ed 3, Baton Rouge, La, 2006, Medical Devices and Systems, CRC Press.
Becker R O: A description of the integrated system of direct currents in the salamander, IRE Trans Biomed Electron 7:202, 1960.
Becker R O: Stimulation of partial limb regeneration in rats, Nature 235:109, 1972.
Becker R O: The bioelectric factors in amphibian limb regeneration, J Bone Joint Surg 43A:643, 1961.
Becker R O, Selden G: The body electric: electromagnetism and the foundation of life, New York City, 1985, William Morrow and Company.
Bembenek P: Akupunktur und bio-resonanz (in German), CO’MED Nr. 6:50, 1998.
Bevk M, Kononenko K, Zrimek T: Relation Between Energetic Diagnoses and DV Images . From the proceedings of the New Science of Consciousness, Ljublana, Russia, October 2000 .
Boyers D G, Tiller W A: Corona discharge photography, J Appl Physics 44:3102, 1973.
Bundzen PV, Korotkov KG, Unestahl L E: Altered states of consciousness: review of experimental data obtained with a multiple techniques approach, J Altern Complement Med 8(2):153-165, 2002.
Caldwell-Bair C: The heart field effect: synchronization of healer-subject heart rates in energy therapy (doctoral dissertation), Fair Grove, M o, 2006, Holos University.
Chiang Lee H, Wah Khong P, Ghista D: Bioenergy based medical diagnostic application based on gas discharge visualization, Conf Proc IEEE Eng Med Biol Soc 2:1533, 2005.
Chu DY et-al: The Effect of External Qi of Qigong on Biomolecular Conformation (III). From the proceedings of the Bridging Worlds and Filling Gaps in the Science of Healing, Chez RA, editor. Hawaii, November 29-December 3, 2001.
Chwirot W B, Dygdala R S, Chwirot S: Quasi-monochromatic-lightinduced photon emission from microsporocytes of larch shows oscillating decay behavior predicted by the electromagnetic model of differentiation, Cytobios 47:137, 1987.
Cohen S, Popp F A: Biophoton emission of the human body, J Photochem Photobiol B, Biol 40:187, 1997.
Cohen S, Popp F A: Biophoton emission of the human body, Indian J Exp Biol 41( 5 ):440, 2003.
Connor M, Schwartz G: Measuring ELF magnetic fields. In Schwartz G, editor: Research Findings at the University of Arizona Center for Frontier Medicine in Biofield Science: A Summary Report. Available at: http://lach.web.arizona.edu/CFMBS_Report.pdf . Accessed September 2007.
Devaraj B, Usa M, Inaba H: Biophotons: ultraweak light emission from living systems, Curr Opin Solid State Mater Sci 2:188, 1997.
Dobrin R et al: Experimental measurements of the human energy field . In Krippner S, Rubin D, editors: The energies of consciousness, New York City, 1975, Gordon and Breach .
Dobrin R et al: Experimental measurements of the human energy field . In Krippner S, editor: Psychoenergetic systems: the interface of consciousness, energy, and matter, New York City, 1979, Gordon and Breach.
Dobson P, O’Keffe E: Investigations into stress and its management using the gas discharge visualization technique, Int J Altern Complement Med 3:12, 2000.
Edwards R et al: Light emission from the human body, Complement Med Res 3:16, 1989.
Edwards R et al: Measurements of human bioluminescence, acupuncture, and electrotherapeutics, Res Int J 15:85, 1990.
Frohlich H: Biological coherence and response to external stimuli, New York City, 1968, Springer-Verlag .
Gurvich A G: Die mitogenetische strahlung, ihre physikalische-chemischen grundlagen und ihre anwendung in biologie und medizin, Jena, Germany, 1959, Veb G Fisher.
Inaba H: Measurement of ultra-weak biophotonic information, Proc Inst Electrostat Japan 22:245, 1998.
Inaba H: Measurement of biophotons from human body, J Int Soc Life Inf Sci 18:448, 2000.
Inyushin V M: Elements of a theory of the biological field (in Russian), Alma-Ata, Kazakhstan, 1978. Kazakh State Department for Higher and Special Academic Education .
Jhaveri A, McCarthy MB, Gronowicz G A: Therapeutic touch affects proliferation and bone formation in vitro, J Altern Complement Med 10( 4 ):723, 2004.
Jones J P: Quantitative Evaluation of Pranic Healing Using Radiation of Cells in Culture. Invited paper presented at the 20th annual meeting of the Society for Scientific Exploration, La Jolla, Calif, 2001.
Jones J P: Oral presentation. Presented at the Biofield Meeting, National Center for Complementary and Alternative Medicine, National Institutes of Health, Bethesda, M d, March 2006 .
Jung HH et al: Left-right asymmetry of biophoton emission from hemiparesis patients, Indian J Exp Biol 41( 5 ):452, 2003.
Jung HH et al: Year-long biophoton measurements: normalized frequency count analysis and seasonal dependency, J Photochem Photobiol B, Biol 78( 2 ):149, 2005.
Kiang J G, Ives J A, Jonas W B: External bioenergy-induced increases in intracellular free calcium concentrations are mediated by N+/Ca2+ exchanger and L-type calcium channel, Mol Cell Biochem 271:51, 2005.
Kim TJ et al: Biophoton emission from fingernails and fingerprints of living human subjects, Acupuncture Electrother Res 27:85, 2002.
Kirlian S, Kirlian V: Photographing and visual observation by means of high frequency currents (in Russian), J Sci Appl Photogr 6 ( 6 ):397, 1961.
Kobayashi M, Devaraj B, Inaba H: Observation of super-Poisson statistics of bacterial (Photobacterium phosphoricum) bioluminescence during the early stage of proliferation, Phys Rev E Stat Nonlin Soft Matter Phys 57:2129, 1998.
Korotkov K: Aura and consciousness, St Petersburg, Russia, 1999, Russian Ministry of Culture, State Editing and Publishing Unit.
Korotkov K: Human energy field: study with GDV bioelectrography, Fair L awn, N J, 2002, Backbone Publishing .
Korotkov K G, Popechitelev E P: [Method for gas-discharge visualization and automation of the system of realizing it in clinical practice], Med Tekh Jan-Feb(1):21, 2002.
Korotkov K, Williams B, Wisneski L A: Assessing biophysical energy transfer mechanisms in living systems: the basis of life processes, J Altern Complement Med 10( 1 ):49, 2004.
Korotkov KG et al: Bioelectrographic correlates of the direct vision phenomenon, J Altern Complement Med 11( 5 ):885, 2005.
Krippner S, Rubin D: Galaxies of life: the human aura in acupuncture and Kirlian photography, New York City, 1973, Gordon and Breach.
Lam F Jr., Tsuei J J, Zhao Z: Studies on the bioenergetic measurement of acupuncture points for determination of correct dosage of allopathic or homeopathic medicine in the treatment of diabetes mellitus, Am J Acupuncture 18:127, 1990.
Liboff A R: Toward an electromagnetic paradigm for biology and medicine, J Altern Complement Med 10( 1 ):41, 2004.
Lin S et al: Measurement of biophoton emission with a single photon counting system, J Altern Complement Med 12:210, 2006.
Lipkind M: Gurwitschs theorie vom biologischen feld, Fusion (Wiesbaden) 8( 4 ):30, 1987.
Mandel P: Energy emission analysis: new application of Kirlian photography for holistic medicine, Berlin, 1986, Synthesis Publishing.
Moss T: The body electric: a personal journey into the mysteries of parapsychological research, bioenergy, and Kirlian photography, Los Angeles, Calif, 1979, JP Tarcher.
Muir J: My first summer in the Sierra, New York City, 1911, Houghton Mifflin.
Oda H: Ryodoraku textbook, Osaka, Japan, 1989, Naniwasha Publishing.
Popp F A: Electromagnetic bio-information, New York City, 1998, Springer-Verlag.
Popp F A: Evolution as the expansion of coherent states . In Zhang C L, Popp F A, Bischof M, editors: Current development of biophysics, Hangzhou, China, 1996, Hangzhou University Press.
Popp FA, Li K H, GuQ, eds: Recent advances in biophoton research and its applications, Singapore and New York, 1992, World Scientific Publishing .
Rademacher P G, Wesener L: Auf der Spur der bio-logik, Tuningen, Germany, 1999, GA U lmer Verlag .
Rubik B: The biofield hypothesis: its biophysical basis and role in medicine, J Altern Complement Med 8( 6 ):703, 2002b.
Rubik B: Can western science provide a foundation for acupuncture? Am Acad Acupunc Rev 5:15, 1993.
Rubik B: Scientific Analysis of the Human Aura . In Heinze R I, editor: Proceedings of the 18th International Conference on the Study of Shamanism and Alternative Modes of Healing. Santa Sabina Center, Dominican University, San Raphael, Calif, September 1-3, 2002a.
Rubik B: The unifying concept of information in acupuncture and other energy medicine modalities, J Altern Complement Med 3(suppl 1):S67, 1997.
Rubik B, Brooks A: Digital high-voltage electrophotographic measures of the fingertips of subjects pre- and post-qigong, Evid Based Integr Med 2( 4 ):24, 2005.
Rubik B et al: In vitro effect of Reiki treatment on bacterial cultures: role of experimental context and practitioner well-being, J Altern Complement Med 12:7, 2006.
Rubik B et al: Manual healing methods. Alternative medicine: expanding medical horizons, Washington, DC, 1994, US Government Printing Office, NIH Publication No. 94-066 .
Russo M et al: Quantitative analysis of reproducible changes in highvoltage electrophotography, J Altern Complement Med 7( 6 ):617, 2001.
Sancier K M: Electrodermal measurements for monitoring the effects of a qigong workshop, J Altern Complement Med 9( 2 ):235, 2003.
Schmidt J et al: Sympathetic nervous system activity during laparoscopic and needlescopic cholecystectomy, Surg Endosc 16( 3 ):476, 2002.
SetoA et al: Detection of extraordinary large bio-magnetic field strength from human hand, Acupuncture Electrother Res Int J 17:75, 1992.
Sheldrake R: A new science of life: the hypothesis of formative causation, London, 1981, Blond and Briggs .
Smith SD : Induction of partial limb regeneration in Rana pipiens by galvanic stimulation, Anat Rec 158(1):89-97, 1967.
Sullivan SG et al: Evoked electrical conductivity on the lung acupuncture points in healthy individuals and confirmed lung cancer patients, Am J Acupuncture 13:261, 1985.
Syldona M, Rein G: The use of DC electrodermal potential measurement and healer’s felt sense to assess the energetic nature of qi, J Altern Complement Med 5( 4 ):329, 1999.
Tiller W A: What are subtle energies? J Soc Sci Explor 7:293, 1993.
Treugut H et al: Reliabilität der energetischen terminalpunktdiagnose (ETD) nach mandel bei kranken, Forsch Komplementärmed 5:224, 1998.
Tsuei JJ et al: A food allergy study utilizing the EAV acupuncture technique, Am J Acupuncture 12( 2 ):105, 1984.
Usa Me t a l: ITEJ Technical Report 15:1, 1991.
Vainshelboim A et al: Observing the behavioral response of human hair to a specific external stimulus using dynamic gas discharge visualization, J Cosmet Sci 55(suppl):S91, 2004.
Van Wijk E P A, Ackerman J, Van Wijk R: Effect of meditation on ultraweak photon emission from hands and forehead, Forsch Komplementarmed Klass Naturheilkd 12:107, 2005.
Van Wijk E P A et al: Anatomic characterization of human ultraweak photon emission in practitioners of transcendental meditation and control subjects, J Altern Complement Med 12( 1 ):31, 2006.
Van Wijk R, Van Wijk EPA: An introduction to human biophoton emission, Forsch Komplementarmed Klass Naturheilkd 12:77, 2005.
Vekaria M: Biophoton emission and intentionality (doctoral dissertation), Encinitas, Calif, 2003, California Institute for Human Science.
Voll R: Twenty years of electroacupuncture diagnosis in Germany: a progress report, Am J Acupuncture 3(19):7, 1975.
Voll R: Verification of acupuncture by means of electroacupuncture according t o Voll, Am J Acupuncture Res Conf 6:5, 1977.
Welch G R: An analogical "field" construct in cellular biophysics: history and present status, Prog Biophys Mol Biol 57:71, 1992.
Welch G R, Smith H A: On the field structure of metabolic spacetime. In Mishra R K, editor: Molecular and biological physics of living systems, Dordrecht, Holland, 1990, Kluwer.
Yount G et al: In vitro test of external qigong, BMC Complement Altern Med 4(15):5, 2004.
Yu T, Tsai HL, Huang M L: Suppressing tumor progression of in vitro prostate cancer cells by emitted psychosomatic power through Zen meditation, Am J Chin Med 31:499, 2003.
Zhang C L: Acupuncture system and electromagnetic standing wave inside body (in Chinese), J Nature 17:275, 1995.
Zhang C L: Standing wave, meridians and collaterals, coherent electromagnetic field and holistic thinking in Chinese traditional medicine (in Chinese), J Yunnan Coll Trad Med 19:27, 1996.
Zimmerman J: Laying-on-of-hands and therapeutic touch: a testable theory, BEMI currents, J Bio-Electro-Magnet Ins 2:8, 1989.

